


For Consumers
Coping With Memory Loss
|
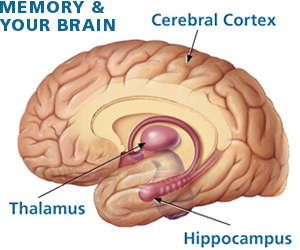
Cerebral Cortex Previously formed memories are thought to be stored in the cerebral cortex. Thalamus Areas of the thalamus are considered to have a role in the formation of new memories partly through their connections with the hippocampus, and partly because the thalamus is considered to be important for mental alertness. Hippocampus The hippocampus is believed to have a critical role in the formation of new memories. Sources: National Institute on Aging and FDA. |
On this page:
- What Can Cause Memory Loss?
- Mild Cognitive Impairment
- Alzheimer's Disease
- Other Diseases That Cause Dementia
- Resources for Coping
- Can Memory Loss Be Prevented?
Everyone has mild memory lapses from time to time. You go from the kitchen to the bedroom to get something, only to find yourself wondering what you needed. You can't find your car keys one day and your reading glasses the next.
Lapses such as these are usually just signs of a normal brain that's constantly prioritizing, sorting, storing, and retrieving all types of information. So how do you know when memory loss is abnormal and warrants evaluation by a health professional? Here are some questions to consider:
- Does the memory loss disrupt daily living? "If memory loss prevents someone from doing activities that they had no trouble handling before—like balancing a checkbook, keeping up with personal hygiene, or driving around—that should be checked," says John Hart, Jr., M.D., professor of behavioral and brain sciences at the University of Texas at Dallas and medical science director at the Center for BrainHealth.
- How often do memory lapses occur? It's one thing to occasionally forget where you parked your car, but it's not normal to forget where you parked every day or to forget appointments over and over. Frequent memory lapses are likely to be noticeable because they tend to interfere with daily living.
- What kinds of things are being forgotten? "It's normal to forget the name of someone you just met, but may not be normal to permanently forget the name of a close friend or relative," Hart says. "It also may not be normal to never remember meeting a person after you have spent a great deal of time with them." Most people have trouble remembering some details of a conversation, but forgetting whole conversations could signal a problem. Other red flags: frequently repeating yourself or asking the same questions in the same conversation.
- Are there signs of confusion? Serious memory lapses may cause individuals to get lost in a familiar place or put something in an inappropriate place because they can't remember where it goes. Putting the car keys in the refrigerator is an example.
- Is the memory loss getting worse? Memory loss that gets progressively worse over time should be evaluated by a health professional.
What Can Cause Memory Loss?
Anything that affects cognition—the process of thinking, learning, and remembering—can affect memory. Doctors use a combination of strategies to gain better insight into what's going on, says Ranjit Mani, M.D., a neurologist and medical reviewer in the Food and Drug Administration's (FDA's) Division of Neurology Products.
|
Ranjit Mani, M.D., is a medical reviewer in FDA's Division of Neurology Products. |
Doctors evaluate memory loss by taking a medical history, asking questions to test mental ability, conducting a physical and neurological examination, and performing blood and urine tests. Brain imaging, using computerized axial tomography (CAT) scans or magnetic resonance imaging (MRI), can help to identify strokes and tumors, which can sometimes cause memory loss. "The goal is to rule out factors that are potentially reversible and determine if the memory loss is due to a more serious brain disease," Mani says.
Causes of memory loss, some of which can occur together, include the following:
- Medications. Examples of medications that can interfere with memory include over-the-counter and prescription sleeping pills, over-the-counter antihistamines, anti-anxiety medications, antidepressants, some medications used to treat schizophrenia, and pain medicines used after surgery.
- Alcohol and illicit drug use. Heavy alcohol use can cause deficiencies in vitamin B1 (thiamine), which can harm memory. Both alcohol and illicit drugs can change chemicals in the brain that affect memory.
- Stress. Stress, particularly due to emotional trauma, can cause memory loss. In rare, extreme cases, a condition called psychogenic amnesia can result. "This can cause someone to wander around lost, unable to remember their name or date of birth or other basic information," Mani says. "It usually resolves on its own."
- Depression. Depression, which is common with aging, causes a lack of attention and focus that can affect memory. "Usually treating the depression will improve mood and the memory problems may then also improve," Mani says.
- Head injury. A blow to the head can cause a loss of consciousness and memory loss. "Memory loss from head trauma typically stays the same or gradually gets better, but not worse," Mani says.
- Infections. People with HIV, tuberculosis, syphilis, herpes, and other infections of the lining or substance of the brain may experience memory problems.
- Thyroid dysfunction. An underactive or overactive thyroid can interfere with remembering recent events.
- Sleep deprivation. Lack of quality sleep—whether from stress, insomnia, or sleep apnea—can affect memory.
- Nutritional deficiencies. Deficiencies of vitamins B1 and B12 can affect memory. Such deficiencies can be treated with a pill or an injection.
- Normal aging. As part of the normal aging process, it can be harder for some people to recall some types of information, such as the names of individuals.
- Mild cognitive impairment. Mild cognitive impairment (MCI) is a condition characterized by a memory deficit beyond that expected for age, which is not sufficient to impair day-to-day activities.
- Dementia. Dementia is a term used for a condition in which there is increasing impairment of memory and other aspects of thinking that are sufficiently severe to impair day-to-day activities. There are many causes of dementia, but the most common by far is Alzheimer's disease (AD), in which there is a progressive loss of brain cells accompanied by other abnormalities of the brain. A diagnosis of AD is made by confirming that a patient has dementia and by excluding other conditions, such as brain tumors, vitamin deficiencies, and hypothyroidism.
Mild Cognitive Impairment
People with MCI have memory impairments, but otherwise function well and don't meet the clinical criteria for dementia. Whereas normal memory loss associated with aging may involve forgetting a name, memory loss associated with MCI is more severe and persistent.
MCI is often a transition stage between normal aging and more serious problems caused by AD. Most, but not all, people with MCI get worse. According to some studies, each year about 12 to 15 percent of people with MCI develop AD.
"Some people never decline in five years and with others, we might see a decline in the third year," says Reisa Sperling, M.D., associate professor of neurology at Harvard Medical School and director of clinical research at the Memory Disorders Unit at Brigham and Women's Hospital. "In older people with MCI, if the memory loss is slowly getting worse, the chances of developing AD are about 60 percent to 70 percent."
Research is under way on whether the drugs approved to treat symptoms of AD may help some people with MCI. Scientists hope that some day, accurate and early evaluation and treatment of people with MCI may help prevent further cognitive decline.
Alzheimer's Disease
AD is the most common form of dementia in people older than age 65, and affects more than 5 million Americans, according to the Alzheimer's Association. AD is a progressive, neurodegenerative disease characterized in the brain by abnormal protein deposits (amyloid plaques) and tangled bundles of fibers within nerve cells (neurofibrillary tangles). The biggest risk factors are age and family history. Having a history of serious concussion is also a risk factor.
AD gradually destroys a person's memory and ability to learn, reason, make judgments, communicate, and carry out daily activities. Memory loss becomes severe and is marked by disorientation, general confusion, and an inability to recall recent events. A person with mild-to-moderate AD may remember things that happened to them a long time ago, but they might get lost easily in a familiar place. People with AD may also experience changes in personality and behavior, such as withdrawal and suspicion. They eventually experience a loss of speech and movement, incapacitation, and death. Some facts about AD treatment follow:
- Most clinical trials of drug treatments for memory loss focus on people with AD.
- Five drugs are approved by FDA to treat the symptoms of AD, but there is no cure for the disease.
- Four drugs are known as cholinesterase inhibitors and are thought to work in a similar way. Cognex (tacrine), Exelon (rivastigmine), and Razadyne (galantamine) are approved for mild-to-moderate AD. Aricept (donepezil) is approved to treat all degrees of severity of the disease—from mild to severe. Cholinesterase inhibitors prevent the breakdown of acetylcholine, a chemical that nerves use to communicate with each other. "These drugs may help delay or decrease the severity of symptoms for a limited time in some people," says Susan Molchan, M.D., formerly program director for the Alzheimer's Disease Neuroimaging Initiative project at the National Institute on Aging (NIA), part of the National Institutes of Health. Side effects of cholinesterase inhibitors are gastrointestinal, such as nausea and diarrhea.
- Namenda (memantine), approved for moderate-to-severe AD, is believed to block the action of glutamate, a brain chemical that may be overactive in people with AD. Namenda may help some patients maintain certain daily functions a little longer. Common side effects include dizziness, headache, constipation, and confusion. Sometimes, Namenda is prescribed along with a cholinesterase inhibitor.
- Behavioral symptoms of AD may include agitation, sleeplessness, anxiety, and depression, which can be treated.
- Inhibiting and/or decreasing amyloid is an intense area of research because amyloid is the major component of the plaques that develop in the brains of people with AD and is associated with nerve cell death. Drugs called secretase inhibitors are being developed and tested to block beta-amyloid formation. Also under study is immunotherapy against beta amyloid—it's possible that a vaccine may help reduce deposits of amyloid. NIA is recruiting patients for a study to determine if a type of protein to reduce brain amyloid slows the rate or prevents the decline of dementia in people with mild-to-moderate AD. For more information on the study, known as the Gammaglobulin Alzheimer's Partnership Study (GAP), visit the Alzheimer's Disease Education and Referral Center Web site or call the center at (800) 438-4380.
Other Diseases That Cause Dementia
Dementia is diagnosed when two or more brain functions, such as memory and language skills, are significantly impaired, according to criteria set forth by the National Institute of Neurological Disorders and Stroke. In practice, doctors use the same drugs that are used to treat AD to treat some other types of dementia.
Vascular dementia. In people who have vascular dementia, also called multi-infarct dementia, arteries to the brain become blocked or narrowed. As a result, changes in the blood supply to the brain occur or multiple strokes disrupt blood flow to the brain. Symptoms may be similar to those of AD, although they usually occur more abruptly. Treatment focuses on preventing future strokes by controlling risk factors such as smoking, diabetes, and high blood pressure.
Lewy body dementia. This progressive brain disease is caused by a buildup of protein deposits called Lewy bodies. It involves progressive cognitive decline, problems with alertness and attention, recurrent visual hallucinations, and motor problems similar to those seen with Parkinson's disease, such as rigidity. Treatment aims to control symptoms of the disorder. Antipsychotic medications for hallucinations aren't typically prescribed because there is a risk of the hallucinations becoming worse.
Parkinson's disease with dementia. Parkinson's disease results from the loss of dopamine-producing brain cells. The primary symptoms are trembling in the hands, arms, legs, jaw, and face; body stiffness; and slowness of movement and impaired balance and coordination. Memory loss sometimes occurs with late-stage Parkinson's disease. Exelon (rivastigmine), which is approved for mild-to-moderate AD, is also approved by FDA for the treatment of dementia with Parkinson's disease.
Frontotemporal dementia. This type of dementia is associated with the shrinking of the frontal and temporal anterior lobes of the brain. Symptoms involve either impulsive or listless behavior, and may include socially inappropriate behavior. Some forms of frontotemporal dementia consist of progressive loss of language functions. No treatment has been shown to slow the progression. Antidepressants and behavior modification may improve some symptoms.
Huntington's disease. This inherited brain disorder causes uncontrolled movements, loss of memory and other cognitive problems, and emotional disturbance. Some early symptoms are mood swings, depression, and difficulty learning new things and remembering facts. Medications help control emotional and movement problems.
Creutzfeldt-Jakob disease (CJD). In the early stages of this rare, degenerative brain disorder, people may experience failing memory, behavioral changes, lack of coordination, and visual disturbances. Mental impairment becomes rapidly more severe as the illness progresses. There is no drug to cure or control CJD, but some drugs may help with symptoms.
Resources for Coping
Coping with memory loss can be frustrating for both the person affected and family members and caregivers. Some families use memory aids to help quality of life, such as color coding and labeling items in the home with safety notes and directions for use, and using alarms and talking clocks to keep track of time and remember medication doses. Families also may experience anger, exhaustion, irritability, and other symptoms of caregiver stress.
Alzheimer's Association. Resources of the Alzheimer's Association include an online message board; a 24/7 toll-free number; information on legal, financial, and living-arrangement decisions; and referrals to local community programs. Services include CareFinder, an interactive tool to help you choose home and residential care providers, and Safe Return, a program that helps when a person with AD or a related dementia wanders and becomes lost.
Alzheimer's Disease Education and Referral Center. A service of NIA. Information specialists can answer questions and offer free publications on home safety tips, caregiving tips, and information on the diagnosis and treatment of AD and related disorders, and ongoing research. A joint NIA and FDA effort maintains the Alzheimer's Disease Clinical Trials Database.
Family Caregiver Alliance. This alliance offers online discussion groups and caregiver information in English, Spanish, and Chinese, as well as fact sheets, including the Caregiver's Guide to Understanding Dementia Behaviors.
Can Memory Loss Be Prevented?
|
'Social interaction … has been associated with a lower risk of dementia.' |

There is no conclusive evidence that the herb ginkgo biloba prevents memory loss. And research has shown that the combination of estrogen and progestin increased the risk of dementia in women older than age 65.
So what can you do to prevent memory loss? Clinical trials are under way to test specific interventions. While those tests are being conducted, you may want to consider hints from animal and observational studies of promising approaches. These steps are already beneficial in other ways and may help reduce the risk of developing memory problems.
- Lower cholesterol and high blood pressure. A number of studies in recent years have suggested that vascular diseases—heart disease and stroke—may contribute to the development of AD, the severity of AD, or the development of multi-infarct dementia (also called vascular dementia).
- Don't smoke or abuse alcohol. According to a research report from Harvard Medical School, "Improving Memory: Understanding Age-Related Memory Loss," smokers perform worse than nonsmokers in studies of memory and thinking skills. Heavy alcohol use can also impair memory.
- Get regular exercise. Physical activity may help maintain blood flow to the brain and reduce risk factors associated with dementia.
- Maintain healthy eating habits. According to a study published in the Oct. 24, 2006, issue of Neurology, eating vegetables may help slow down the rate of cognitive change in adults. Researchers studied 3,718 residents in Chicago who were older than age 65. Of the types of vegetables, green leafy vegetables had the strongest association with slowing the rate of cognitive decline. Also reducing foods high in saturated fat and cholesterol and eating fish with beneficial omega-3 fatty acids, such as salmon and tuna, may benefit brain health. An NIA-funded clinical trial to test the effects of omega-3 fatty acids in people with AD is now recruiting patients nationwide.
- Maintain social interactions. Social interaction can help reduce stress levels and has been associated with a lower risk of dementia. In the February 2007 issue of the Archives of General Psychiatry, researchers found that loneliness is associated with an increased risk of late-life dementia.
- Keep your brain active. Some experts suggest that challenging the brain with such activities as reading, writing, learning a new skill, playing games, and gardening stimulates brain cells and the connections between the cells, and may be associated with a lower risk of dementia.
Sources: NIH, Alzheimer's Association
This article appears on FDA's Consumer Updates page, which features the latest on all FDA-regulated products.
Updated: January 6, 2010

