Epidemiology
Dengue fever (DF) is caused by any of four closely related viruses, or serotypes: dengue 1-4. Infection with one serotype does not protect against the others, and sequential infections put people at greater risk for dengue hemorraghic fever (DHF) and dengue shock syndrome (DSS).
Transmission of the Dengue Virus
Dengue is transmitted between people by the mosquitoes Aedes aegypti and Aedes albopictus, which are found throughout the world. Insects that transmit disease are vectors. Symptoms of infection usually begin 4 - 7 days after the mosquito bite and typically last 3 - 10 days. In order for transmission to occur the mosquito must feed on a person during a 5- day period when large amounts of virus are in the blood; this period usually begins a little before the person become symptomatic. Some people never have significant symptoms but can still infect mosquitoes. After entering the mosquito in the blood meal, the virus will require an additional 8-12 days incubation before it can then be transmitted to another human. The mosquito remains infected for the remainder of its life, which might be days or a few weeks.
In rare cases dengue can be transmitted in organ transplants or blood transfusions from infected donors, and there is evidence of transmission from an infected pregnant mother to her fetus. But in the vast majority of infections, a mosquito bite is responsible.
In many parts of the tropics and subtropics, dengue is endemic, that is, it occurs every year, usually during a season when Aedes mosquito populations are high, often when rainfall is optimal for breeding. These areas are, however, additionally at periodic risk for epidemic dengue, when large numbers of people become infected during a short period. Dengue epidemics require a coincidence of large numbers of vector mosquitoes, large numbers of people with no immunity to one of the four virus types (DENV 1, DENV 2, DENV 3, DENV 4), and the opportunity for contact between the two. Although Aedes are common in the southern U. S., dengue is endemic in northern Mexico, and the U.S. population has no immunity, the lack of dengue transmission in the continental U.S. is primarily because contact between people and the vectors is too infrequent to sustain transmission.
Dengue is an Emerging Disease
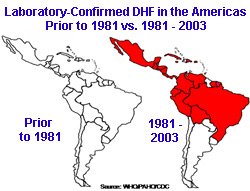
The four dengue viruses originated in monkeys and independently jumped to humans in Africa or Southeast Asia between 100 and 800 years ago. Dengue remained a relatively minor, geographically restricted disease until the middle of the 20th century. The disruption of the second world war – in particular the coincidental transport of Aedes mosquitoes around the world in cargo - are thought to have played a crucial role in the dissemination of the viruses. DHF was first documented only in the 1950s during epidemics in the Philippines and Thailand. It was not until 1981 that large numbers of DHF cases began to appear in the Carribean and Latin America, where highly effective Aedes control programs had been in place until the early 1970s.
Global Dengue
Today about 2.5 billion people, or 40% of the world’s population, live in areas where there is a risk of dengue transmission see WHO/Impact of Dengue. Dengue is endemic in at least 100 countries in Asia, the Pacific, the Americas, Africa, and the Caribbean. The World Health Organization (WHO) estimates that 50 to 100 million infections occur yearly, including 500,000 DHF cases and 22,000 deaths, mostly among children.
Dengue in the United States
Nearly all dengue cases reported in the 48 continental states were acquired elsewhere by travelers or immigrants. (Travel Associated Dengue Infections - United States, 2001- 2004 , Imported Dengue - United States, 1999 and 2000 ) Because contact between Aedes and people is infrequent in the continental U.S., these imported cases rarely result in secondary transmission. The last reported continental dengue outbreak was in south Texas in 2005. (Dengue Hemorrhagic Fever - U.S.- Mexico Border, 2005) A small dengue outbreak occurred in Hawaii in 2001.
Most dengue cases in U.S. citizens occur in those inhabitants of Puerto Rico, the U.S. Virgin Islands, Samoa and Guam, which are endemic for the virus. Dengue and DHF have been a particular challenge in Puerto Rico, where outbreaks have been reported since 1915 and large island-wide epidemics have been documented since the late 1960s. The most recent island-wide epidemic occurred in 2007, when more than 10,000 cases were diagnosed. In Puerto Rico, and most of the Caribbean Basin, the principle dengue vector Ae. aegypti is abundant year-round. Dengue transmission in the Puerto Rico follows a seasonal pattern. Low transmission season begins in March and lasts until June, and high transmission begins in August until November.
Dengue Surveillance in the U.S.
DF and DHF cases have long been reportable by law to public health authorities in 26 states. Beginning in 2009, all nationally diagnosed dengue infections will be reportable to the CDC.
Statistics on cases have been compiled in Puerto Rico since 1915 and, since 1969, CDC’s Dengue Branch, located at San Juan, has operated the island-wide passive dengue surveillance system (PDSS) in partnership with the Puerto Rico Department of Health. PDSS was instrumental in confirming the endemic presence of dengue transmission in Puerto Rico, identifying the first case of DHF in the Americas, and detecting the first cluster of cases of DHF and the first laboratory-confirmed, dengue-related death in Puerto Rico. Instructions and forms for reporting suspected or confirmed cases of dengue are linked below.
Tools and links
- WHO guidelines for the clinical management of dengue infection
- WHO guidelines for treatment of dengue fever/dengue hemorrhagic fever in small hospitals [PDF - 33 pages]
- U.S. Council for State and Territorial Epidemiologist (CSTE) 2009 dengue case definitions [PDF - 15 pages]
Clinical management tools for health care providers
- Clinician’s case management card [PDF - 2 pages]
- Information for health care providers [PDF -4 pages]
Requesting dengue laboratory testing and case reporting
Contact Us:
- Centers for Disease Control and Prevention
Dengue Branch
1324 Calle Cañada
San Juan, Puerto Rico
00920-3860 - 800-CDC-INFO
(800-232-4636)
TTY: (888) 232-6348 - New Hours of Operation
8am-8pm ET/Monday-Friday
Closed Holidays - cdcinfo@cdc.gov
