


Topics in Brief: Methamphetamine Addiction: Progress, but Need to Remain Vigilant
Revised November 2011
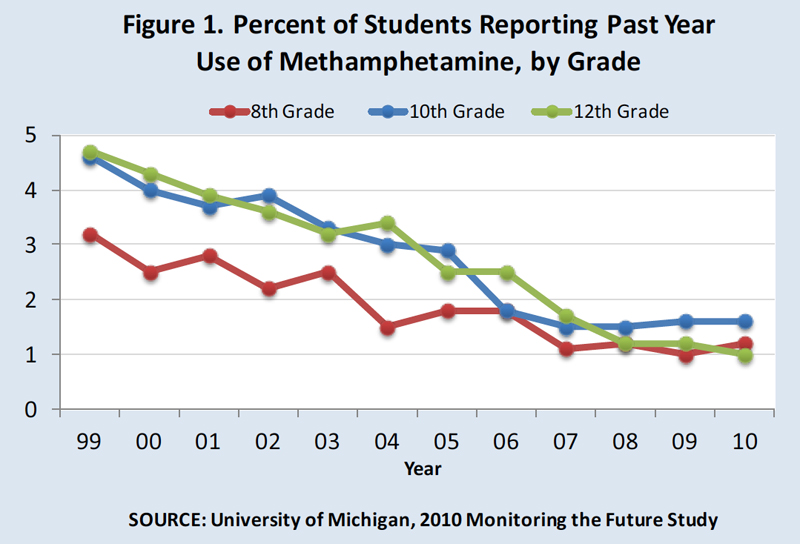
Declines in Methamphetamine Abuse by Youth
- Approximately 13 million people 12 years and older have abused methamphetamine in their lifetimes; in 2010, approximately 353,000 were current users (NSDUH).
- According to NIDA's 2010 Monitoring the Future Survey, the abuse rate among 8th 10th, and 12th graders declined significantly between 1999 and 2007 and has remained unchanged since then (Figure 1).
- Abuse remains noteworthy in certain areas of the country with indicators suggesting particular problems in Hawaii, the West Coast, and the Midwest.
- Methamphetamine's potent addiction liability and destructive health and social consequences make its abuse particularly dangerous.
Methamphetamine acts by increasing the release of dopamine in the brain, which leads to feelings of euphoria. However, this surge of pleasure is followed by a "crash" that often leads to repeated use of the drug and eventually to difficulty feeling any pleasure at all, especially from natural rewards. Long-term methamphetamine abuse also results in many damaging physical and psychiatric effects, such as:
- Addiction
- Violent Behavior
- Anxiety
- Confusion
- Insomnia
- Psychotic symptoms (e.g. paranoia, hallucinations, delusions)
- Cardiovascular problems (e.g. rapid heart rate, irregular heartbeat, increased blood pressure, stroke).
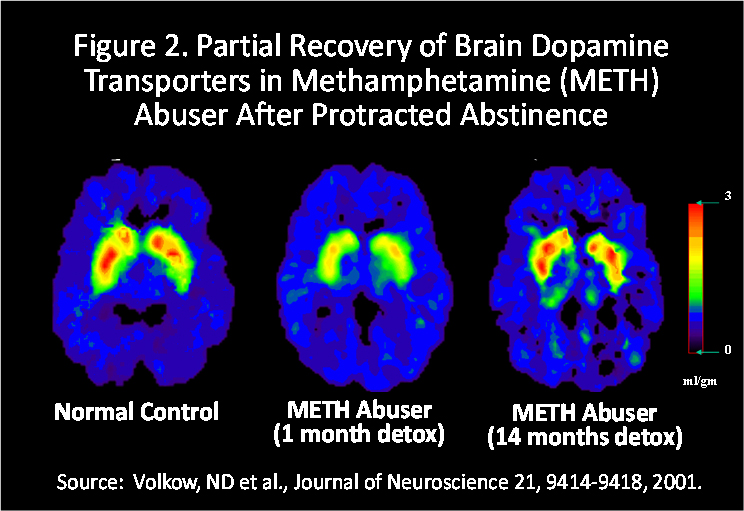
What Does Methamphetamine Do to the Brain?
Methamphetamine's adverse effects on the brain are clear. Imaging studies have demonstrated changes in the dopamine system (important for reward, motivation, and learning) as well as structural and functional deficits in brain areas associated with emotion and memory. These may account for the psychiatric and cognitive problems observed in chronic abusers. Fortunately, some of the methamphetamine-induced deficits in dopamine function have been shown to recover, at least partially, with extended abstinence (Figure 2). But even with the partial recovery found in some brain regions following protracted abstinence, other regions do not show recovery of function—suggesting that long-lasting and even permanent brain changes may result from methamphetamine abuse.
Methamphetamine and HIV
Methamphetamine is inextricably linked with HIV, hepatitis C, and other sexually transmitted diseases. Its abuse increases the risk of contracting HIV not only through the use of contaminated injection equipment, but also through increased risky sexual behaviors and through physiological changes that may favor HIV transmission.
Methamphetamine abuse may also affect HIV disease progression. For example, clinical studies suggest that current methamphetamine abusers on highly active antiretroviral therapy may be at greater risk of developing AIDS than non-users, possibly due to poor medication adherence or interactions between methamphetamine and HIV medications. Similarly, preliminary studies suggest that interactions between methamphetamine and HIV itself may lead to more severe consequences for HIV-positive patients who abuse methamphetamine, including greater brain damage and cognitive impairment. More research is needed to better understand these interactions.
Treatments for Methamphetamine Addiction
Methamphetamine addiction can be successfully treated. For example, the Matrix Model consists of a 16-week intervention that includes intensive group and individual therapy to promote the behavioral changes needed to remain abstinent, prevent relapse, and establish a lifestyle unrelated to drugs. When applied to methamphetamine abusers, the Matrix Model has been shown to significantly reduce drug use (Figure 3).

Motivational Incentives for Enhancing Drug Abuse Recovery (MIEDAR), an incentive-based method for promoting cocaine and methamphetamine abstinence, is another treatment that has demonstrated efficacy in methamphetamine abusers through NIDA's National Drug Abuse Clinical Trials Network.
There are currently no medications approved for the treatment of methamphetamine addiction. However, NIDA has made medications development a high priority. For example, a recent clinical trial revealed that the antidepressant bupropion, marketed as Welbutrin® is effective in reducing methamphetamine abuse in low/moderate users. Additional clinical trials of bupropion, and other medications (e.g., the antidepressant Mirtazapine) are currently underway. NIDA is also pursuing the novel approach of using vaccines, where antibodies are generated against the drug itself, to treat methamphetamine addiction. The antibodies would bind methamphetamine while it is still in the bloodstream, reduce its entry into the brain, and block its rewarding effects.