
General Information About Melanoma
Key Points for This Section
- Melanoma is a disease in which malignant (cancer) cells form in the skin cells called melanocytes (cells that color the skin).
- Melanoma can occur anywhere on the body.
- Unusual moles, exposure to sunlight, and health history can affect the risk of developing melanoma.
- Possible signs of melanoma include a change in the appearance of a mole or pigmented area.
- Tests that examine the skin are used to detect (find) and diagnose melanoma.
- Certain factors affect prognosis (chance of recovery) and treatment options.
Melanoma is a disease in which malignant (cancer) cells form in the skin cells called melanocytes (cells that color the skin).
Melanocytes are found throughout the lower part of the epidermis. They make melanin, the pigment that gives skin its natural color. When skin is exposed to the sun, melanocytes make more pigment, causing the skin to tan, or darken.
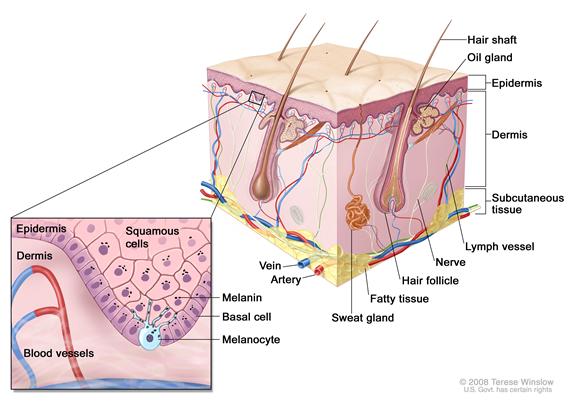
The skin is the body’s largest organ. It protects against heat, sunlight, injury, and infection. The skin has 2 main layers: the epidermis (upper or outer layer) and the dermis (lower or inner layer).
There are 3 types of skin cancer:
When melanoma starts in the skin, the disease is called cutaneous melanoma. Melanoma may also occur in mucous membranes (thin, moist layers of tissue that cover surfaces such as the lips). This PDQ summary is about cutaneous (skin) melanoma and melanoma that affects the mucous membranes. When melanoma occurs in the eye, it is called intraocular or ocular melanoma. (See the PDQ summary on Intraocular (Eye) Melanoma Treatment for more information.)
Melanoma is more aggressive than basal cell skin cancer or squamous cell skin cancer. (See the PDQ summary on Skin Cancer Treatment for more information on basal cell and squamous cell skin cancer.)
Melanoma can occur anywhere on the body.
In men, melanoma is often found on the trunk (the area from the shoulders to the hips) or the head and neck. In women, melanoma forms most often on the arms and legs. Melanoma is most common in adults, but it is sometimes found in children and adolescents. See the PDQ summary on Unusual Cancers of Childhood for more information on melanoma in children and adolescents.)
Unusual moles, exposure to sunlight, and health history can affect the risk of developing melanoma.
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn't mean that you will not get cancer. Talk with your doctor if you think you may be at risk for melanoma. Risk factors for melanoma include the following:
- Having a fair complexion, which includes the following:
- Fair skin that freckles and burns easily, does not tan, or tans poorly.
- Blue or green or other light-colored eyes.
- Red or blond hair.
- Being exposed to natural sunlight or artificial sunlight (such as from tanning beds) over long periods of time.
- Having a history of many blistering sunburns, especially as a child or teenager.
- Having several large or many small moles.
- Having a family history of unusual moles (atypical nevus syndrome).
- Having a family or personal history of melanoma.
- Being white.
Being white or having a fair complexion increases the risk of melanoma, but anyone can have melanoma, including people with dark skin.
Possible signs of melanoma include a change in the appearance of a mole or pigmented area.
These and other symptoms may be caused by melanoma. Other conditions may cause the same symptoms. A doctor should be consulted if any of the following problems occur:
- A mole that:
- changes in size, shape, or color.
- has irregular edges or borders.
- is more than one color.
- is asymmetrical (if the mole is divided in half, the 2 halves are different in size or shape).
- itches.
- oozes, bleeds, or is ulcerated (a hole forms in the skin when the top layer of cells breaks down and the tissue below shows through).
- A change in pigmented (colored) skin.
- Satellite moles (new moles that grow near an existing mole).
For pictures and descriptions of common moles and melanoma, see Common Moles, Dysplastic Nevi, and Risk of Melanoma.
Tests that examine the skin are used to detect (find) and diagnose melanoma.
If a mole or pigmented area of the skin changes or looks abnormal, the following tests and procedures can help find and diagnose melanoma:
- Skin exam: A doctor or nurse checks the skin for moles, birthmarks, or other pigmented areas that look abnormal in color, size, shape, or texture.
- Biopsy: The removal of as much of the abnormal mole or lesion as possible. A pathologist looks at the tissue under a microscope to check for cancer cells. It can be hard to tell the difference between a colored mole and an early melanoma lesion. Patients may want to have their biopsy sample checked by a second pathologist.
A biopsy should be done on any abnormal areas of the skin. These areas should not be shaved off or cauterized (destroyed with a hot instrument, an electric current, or a caustic substance).
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) and treatment options depend on the following:
- The thickness of the tumor and where it is in the body.
- How quickly the cancer cells are dividing.
- Whether there was bleeding or ulceration at the primary site.
- Whether cancer has spread to the lymph nodes or to other places in the body.
- The number of places cancer has spread to in the body and the level of lactate dehydrogenate (LDH) in the blood.
- The patient’s general health.
 Back to Top
Back to Top