Disaster Mental Health Primer: Key Principles, Issues and Questions
NOTE: These materials represent highlights of the kinds of mental-health related information that might be beneficial in a disaster. Because of their brevity, they do not provide an exhaustive, formal review or compilation of the wealth of available knowledge on disaster mental health. This is a starting point. There are companion pieces that provide similar information for city, county and state Public Health officials and as a general primer. Sources of additional information are listed at the end of this document.
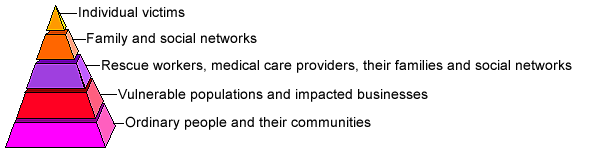
The Impact Pyramid (The victim count only represents the tip of the iceberg.)
Guiding Principles (It is helpful to keep these points in mind when preparing for or responding to a disaster.)
- No one who experiences a disaster is untouched by it.
- Most people pull together and function during and after a disaster, but their effectiveness is diminished.
- Mental health concerns exist in most aspects of preparedness, response and recovery.
- Disaster stress and grief reactions are “normal responses to an abnormal situation.”
- Survivors respond to active, genuine interest and concern.
- Disaster mental health assistance is often more practical than psychological in nature (offering a phone, distributing coffee, listening, encouraging, reassuring, comforting).
- Disaster relief assistance may be confusing to disaster survivors. They may experience frustration, anger, and feelings of helplessness related to Federal, State, and non-profit agencies’ disaster assistance programs. They may reject disaster assistance of all types.
Phases of a Disaster (General Principles. No precise, universal timeline exists. Responses vary by disaster. These phases first were observed/described in natural disasters.)
- Warning of Threat: Ranges from no advance notice (suicide bomber) to weeks (hurricane)
- Impact: Actual onset of disaster Varies. BT has fuzzy beginning/end; bombing is precise
- Rescue or Heroic: People watch out for, protect, even risk own safety to save strangers
- Remedy or Honeymoon: People initially pitch in and collaborate for the collective good
- Inventory: External resources begin to come online—people watch what goes where
- Disillusionment: Resource allocation often seen as too little too late, poorly distributed
- Reconstruction and Recovery: People move beyond self interests and start to rebuild
Factors That Determine the Stressfulness of a Disaster (Individual responses are a function of the interplay of multiple factors.)
- Features of the Disaster
- Familiarity with the event
- Avoidability of the event
- Suddenness of its onset
- Intensity of its impact
- Course and duration of the event
- Degree to which it can be controlled
- Community or Societal Factors
- Previous level of community resources
- Community’s level of preparedness
- Extent and nature of damage don
- Community’s experience with such an event
- Consequent social/political unrest
- Availability of resources to rebuild
- Characteristics of the Individuals Involved
- Actual losses (and threat of loss)
- Previous experience with similar events
- Level of background stress in one’s life
- Physical or psychological closeness to event
- Effectiveness of one’s coping mechanisms
- Nature and extent of available social support
Severity of Psychological Reaction After a Traumatic Event (Most people affected by a traumatic event “recover” without external intervention.)

Potential Risk Groups (Certain individuals/groups are more vulnerable than others.)
- Age groups (Infants, children and seniors)
- Cultural and Ethnic Groups (immigrants, non-English speakers, undocumented aliens etc.)
- Low-visibility groups (homeless, mobility-impaired, unemployed, mentally-challenged etc.)
- People with Serious and Persistent Mental Illness
- People in Group Facilities (hospitals, nursing homes, prisons)
- Human Service, Healthcare and Disaster Relief Workers
Survivor’s Needs & Reactions (While people respond differently, there are common needs.)
- A concern for basic survival
- Grief over loss of loved ones and loss of valued/meaningful possessions
- Fear and anxiety about personal safety and physical safety of loved ones
- Sleep disturbances, often including nightmares and imagery from the disaster
- Concerns about relocation and the related isolation or crowded living conditions
- A need to talk, often repeatedly, about events and feelings associated with the disaster
- A need to feel one is a part of the community and its recovery efforts
Reactions that Signal Possible Need for Mental Health Referral (Many responses to trauma are expected, but some require extra attention and concern.)
- Disorientation (dazed, memory loss, unable to give date/time or recall recent events…)
- Depression (pervasive feeling of hopelessness & despair, withdrawal from others…)
- Anxiety (constantly on edge, restless, obsessive fear of another disaster…)
- Mental Illness (hearing voices, seeing visions, delusional thinking…)
- Inability to care for self (not eating, bathing, changing clothing or handling daily life)
- Suicidal or homicidal thoughts or plans
- Problematic use of alcohol or drugs
- Domestic violence, child abuse or elder abuse
Common Disaster Worker Stress Reactions (See list in: “Disaster Mental Health for Responders: Key Principles, Issues and Questions”)
Stress Basics (A quick review to help keep stress in perspective.)
Stress is:
- Normal
- Necessary
- Productive and destructive
- Acute and delayed
- Cumulative
- Identifiable
- Preventable (Much stress is); Manageable (Most stress is)
Some of the Sources of Information Used in this Overview
The Centers for Public Health Preparedness Program
American Psychiatric Association
National Center for Post Traumatic Stress Disorder
The National Child Traumatic Stress Network
Uniformed Services University of the Health Sciences
Contact Us:
- Centers for Disease Control and Prevention
1600 Clifton Rd
Atlanta, GA 30333 - 800-CDC-INFO
(800-232-4636)
TTY: (888) 232-6348 - Contact CDC-INFO


