
24
24
Co-Lead Agencies: | Centers for Disease Control and Prevention |
[Note: The Healthy People 2010 Information Access Project provides dynamic, pre-formulated PubMed searches for selected objectives in this focus area so that current information and evidence-based strategies related to these objectives are easier to find. The National Library of Medicine has also provided PubMed links to available references that appear at the end of this focus area document.]
Contents
 Chronic Obstructive Pulmonary Disease
Chronic Obstructive Pulmonary Disease
Interim Progress Toward Year 2000 Objectives
Healthy People 2010—Summary of Objectives
Healthy People 2010 Objectives
Chronic Obstructive Pulmonary Disease
Related Objectives From Other Focus Areas
Promote respiratory health through better prevention, detection, treatment, and education efforts.
Asthma, chronic obstructive pulmonary disease (COPD), and obstructive sleep apnea (OSA) are a significant public health burden to the United States.[1] Specific methods of detection, intervention, and treatment exist that may reduce this burden. Several behaviors and diseases that affect the respiratory system, such as tuberculosis, lung cancer, acquired immunodeficiency syndrome (AIDS), pneumonia, occupational lung disease, and smoking, are covered in other chapters. (See Focus Area 3. Cancer, Focus Area 13. HIV, Focus Area 14. Immunization and Infectious Diseases, Focus Area 20. Occupational Safety and Health, Focus Area 25. Sexually Transmitted Diseases, and Focus Area 27. Tobacco Use.) Certain other important respiratory diseases, such as respiratory distress syndromes, sarcoidosis, and chronic sinusitis, which are difficult to define, detect, prevent, or treat, are not discussed in this chapter. Their omission, however, is not a reflection on the magnitude of the health problems associated with them.
Asthma and COPD are among the 10 leading chronic conditions causing restricted activity. After chronic sinusitis, asthma is the most common cause of chronic illness in children.[2] Methods are available to treat these respiratory diseases and promote respiratory health.
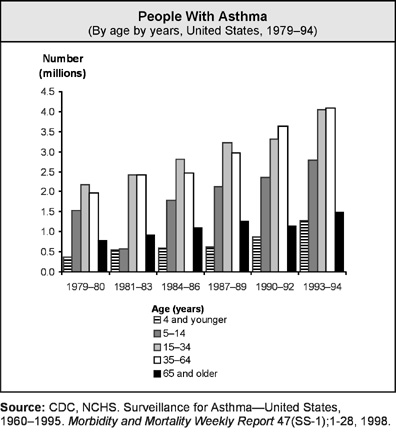
Asthma is a serious and growing health problem. An estimated 14.9 million persons in the United States have asthma.[3] The number of people with asthma increased by 102 percent between 1979–80 and 1993–94.[4]
Asthma is responsible for about 500,000 hospitalizations,3 5,000 deaths,3 and 134 million days4 of restricted activity a year. Yet most of the problems caused by asthma could be averted if persons with asthma and their health care providers managed the disease according to established guidelines. Effective management of asthma comprises four major components: controlling exposure to factors that trigger asthma episodes, adequately managing asthma with medicine, monitoring the disease by using objective measures of lung function, and educating asthma patients to become partners in their own care.2, [5] Such prevention efforts are essential to interrupt the progression from disease to functional limitation and disability and to improve the quality of life for persons with asthma.
In 1996, asthma was the 10th most common principal diagnosis in emergency department (ED) visits.3 Among diseases commonly seen in outpatient departments, asthma was the ninth most frequent diagnosis in 1996.[6] In 1995, some 9 million physician office visits were made for asthma.6 From 1990 to 1992, persons with asthma spent an estimated 64 million days in bed because of asthma, ranking asthma as the fourth highest chronic health condition.4 The proportion of people with asthma who are limited in activity increased slightly from 19.4 percent in 1986–88 to 19.6 percent in 1994–96.[7]
Direct medical expenditures for asthma amounted to $3.64 billion in 1990, and indirect economic losses accounted for an additional $2.6 billion.[8] Of direct medical care costs, approximately 57 percent was spent on hospitalizations ($1.6 billion), outpatient hospital visits ($190 million), and ED visits ($295 million). Physician-related services accounted for 14 percent of the total expenditures, including $347 million for outpatient services. Prescription medications represented 30 percent of direct medical costs. Such facts highlight the significant cost of hospital care for asthma, compared to the more frequently used and less costly outpatient and pharmaceutical services.
Indirect costs—nonmedical economic losses such as days missed from work or school, caregiver costs, travel and waiting time, early retirement due to disability, and premature death—account for slightly less than 50 percent of the total costs of asthma. Data suggest that the uneven distribution of costs of asthma relates to nonscheduled acute or emergency care, indicating poor asthma management and suboptimal outcomes.[9], [10]
Environmental and occupational factors contribute to illness and disability from asthma. Decreases in lung function and a worsening of asthma have been associated with exposure to allergens, indoor pollutants (for example, tobacco smoke), and ambient air pollutants (for example, ozone, sulfur dioxide, nitrogen dioxide, acid aerosols, and particulate matter).[11], [12] Approximately 25 percent of children in the United States live in areas that exceed the Federal Government’s standard for ozone.[13] Occupational factors cause or trigger asthma episodes in 5 to 30 percent of adults with the disease.[14] Environmental factors are associated with upper respiratory infections that contribute to illness and disability in children and adults.[15] (See Focus Area 8. Environmental Health.)
Within the U.S. population, the health, economic, and social burdens of asthma vary. Disproportionate rates of death, hospitalization, ED use, and disability from asthma occur in certain age, gender, racial, and ethnic groups.
While the number of adults with asthma is greater than the number of children with asthma, the asthma rate is rising more rapidly in preschool-aged children than in any other group.1 In 1995, the rate of self-reported asthma among children and adolescents under age 18 years was 7.5 percent, compared to 5.7 percent among the general population. The rates were higher in boys under age 18 years than in girls in the same age group. The rates of self-reported asthma were higher for women (6.7 percent) than men (5.2 percent) and higher for African Americans (6.7 percent) than whites (5.6 percent).1 Among adults, women of all races have higher rates of illness and death from asthma than men.[16]
Death from asthma is two to six times more likely to occur among African Americans and Hispanics than among whites.1 Although the number of deaths annually from asthma is low compared to other chronic diseases, the death rate for children aged 5 to 14 years and young adults aged 15 to 34 years doubled from 1979–80 to 1993–95 (from 1.5 to 3.7 deaths per million children aged 5 to 14 years and 2.8 to 6.3 deaths per million persons aged 15 to 34 years).1 In 1993–95,death rates are slightly higher overall in women than in men.1
Rates of hospitalization for asthma demonstrate similar variations. Rates for African Americans are almost triple those for whites. Rates are higher among women than among men.1 Asthma hospitalization rates have increased dramatically among children under age 5 years. From 1980 to 1993, the rate increased from 36 to 65 children hospitalized per 10,000 children under age 1 year. Some of this increase may be related to changes in diagnostic practices and changes in coding and reimbursement, but a large portion represents a true increase in illness and disability.
In the inner city, patients frequently use EDs for asthma care. In 1993 and 1994, African Americans were four times more likely than whites to visit an ED because of asthma.1 Asthma patients in general and high-risk inner-city patients—in particular, those with a history of severe asthma who were hospitalized or visited the ED for asthma within the previous 2 years—need to be able to recognize the signs and symptoms of uncontrolled asthma and know how to respond appropriately.
The economic burden of asthma disproportionately affects patients with severe disease. Socioeconomic status, particularly poverty, appears to be an important contributing factor to asthma illness, disability, and death. In the United States, the rate of asthma cases for nonwhites is only slightly higher than for whites, yet the death, hospitalization, and ED-visit rates for nonwhites are more than twice those for whites.1 Although reasons for these differences are unclear, they likely result from multiple factors: high levels of exposure to environmental tobacco smoke, pollutants, and environmental allergens (for example, house dust mites, cockroach particles, cat and dog dander, and possibly rodent dander and mold); a lack of access to quality medical care; and a lack of financial resources and social support to manage the disease effectively on a long-term basis.[17] Research into the role of socioeconomic factors is needed to identify additional prevention opportunities.
Scientific research has led to greater asthma control than was available in the early 1980s.5 Effective management of asthma includes four components: avoiding or controlling the factors that may make asthma worse (for example, environmental and occupational allergens and irritants), taking appropriate medications tailored to the severity of the disease, objective monitoring of the disease by the patient and the health care professional, and actively involving the patient in managing the disease.5 Effective asthma management reduces the need for hospitalizations and urgent care visits (in either an ED or physician’s office) and enables patients to enjoy normal activities.[18], [19]
Advances in human genetics related to asthma are expected to provide better information about the contribution of genetic variation to the development of disease when people are exposed to certain environmental factors and variation in individual response to therapy. The use of this genetic information will improve targeted disease prevention and health management strategies for respiratory diseases.
Patient education is one of four components of effective asthma management.5 Patients who are taught asthma self-management skills are able to manage and control their disease better than patients who do not receive education.5 Patients need to learn to work with health care providers to optimize asthma care. Thus, both patients and health care providers need to be trained and educated on effective asthma management. Health outcomes for asthma—illness, disability, quality of life, and death—are related directly to the actions of health care professionals and patients. The National Asthma Education and Prevention Program (NAEPP) provides guidelines for diagnosis and management that should be incorporated into the curricula of health professional schools.5, [20] Currently, there are no national data systems for tracking the training of health care providers in asthma management. Therefore, the issue is not covered in this focus area’s objectives. It represents an important research and data collection agenda for the coming decade. In addition, research to identify the primary causes of development of asthma is a high priority. Such research can provide a scientific basis for efforts to prevent the development of asthma.
To control asthma effectively, asthma patients, particularly those on daily medication, need an asthma action plan developed under their physician’s guidance. The plan spells out when and how to take medicines correctly, as well as what to do when asthma worsens. The treatment of persistent asthma emphasizes daily long-term therapy aimed at the underlying inflammation and preventing symptoms, rather than relying solely on treating symptoms with short-acting inhaled medication, such as a beta agonist medication. Use of more than one canister of the short-acting inhaled beta agonist medication per month is an indication of uncontrolled asthma and the need to start or increase long-term preventive therapy. Patients also need to work with health care providers during followup visits, particularly after being hospitalized, to make sure they understand and are able to follow the long-term management plan.
Working with local community groups to mobilize community resources for a comprehensive, culturally and linguistically competent approach to controlling asthma among high-risk populations is a priority. From a community-based perspective, States need to track occupational and environmental factors that cause or trigger asthma episodes. Such surveillance efforts should include collecting State-based data on the proportion of the population with asthma and monitoring occupational and environmental exposures and their impact on illness and disability related to asthma. Efforts directed to improving the environmental management of asthma also include reducing exposure to allergens and irritants, such as environmental tobacco smoke, and outdoor air pollution from ozone, sulfur dioxide, and particulate diesel matter. (See Focus Area 8. Environmental Health.)
Professional organizations, lay volunteer groups, Federal agencies, and the private sector have worked together and with NAEPP to implement a spectrum of asthma programs at national and local community levels. For example, numerous publications, media campaigns, and conferences target various audiences. Intensified efforts are planned to reach primary care providers, patients, and school personnel.16, 20 A high-level work group convened by the U.S. Department of Health and Human Services in 1997 assessed the most urgent needs for tackling the growing problem of asthma. The work group’s departmentwide strategic plan, Action Against Asthma, identified opportunities and presented a coordinated approach for improving asthma prevention and management.16
COPD includes chronic bronchitis and emphysema—both of which are characterized by irreversible airflow obstruction and often exist together. Similar to asthma, COPD may be accompanied by an airway hyperresponsiveness. Most patients with COPD have a history of cigarette smoking. COPD worsens over time with continued exposure to a causative agent—usually tobacco smoke or sometimes a substance in the workplace or environment.
COPD occurs most often in older people. As much as 10 percent of the population aged 65 years and older is estimated to have COPD.2 COPD has a major impact on health care, illness, disability, and death in the older population, and the magnitude of the problem is growing. Since 1980, the prevalence and age-adjusted death rate for COPD increased more than 30 percent.2, [21], [22] Most of the increase occurred in people over age 65 years. Taking into account the expected aging of the U.S. population over the next 10 to 30 years as well as the improved management of other smoking-related diseases, any decline in the proportion of persons with COPD is unlikely without substantial changes in risk factors, mainly reductions in cigarette smoking. This is important for both men and women, given the modest decline in cigarette smoking rates from 1990 to 1995.22
Between 80 and 90 percent of COPD is attributable to cigarette smoking. However, not all smokers develop COPD, and not all patients with COPD are smokers or have smoked in the past.[23], [24] Individual susceptibility to the adverse health effects of cigarette smoke on the lung appears to vary within the general population. Some 10 to 15 percent of smokers show a rate of decline in lung function that will result in COPD with severe disability. Smoking cessation is the only treatment that slows the decline. Susceptible smokers who stop smoking do not regain lost lung function,[25] but the rate of loss will return to what is normal for a nonsmoker.
How cigarette smoking causes COPD is an active area of research. The development of COPD—in particular, emphysema—is thought to be due to a chemical imbalance in the lungs caused by cigarette smoke.[26] In some individuals, emphysema occurs because of a genetic deficiency. Emphysema due to genetic deficiency, called familial emphysema, occurs even in nonsmokers, but smoking hastens its occurrence. Familial emphysema probably accounts for less than 5 percent of all cases of COPD.[27]
Smoking and occupational exposures together cause respiratory diseases and lung cancer.[28], [29] Miners, firefighters, metal workers, grain handlers, cotton workers, paper mill workers, agricultural workers, construction workers who handle cement, and others employed in occupations associated with prolonged exposure to dusts, fumes, or gases develop significant airflow obstruction, coughing, phlegm, dyspnea, wheezing, and reduced lung function.27, 29, [30]
Population studies have shown that chronic exposure to air pollution has an independent adverse effect on lung function.[31], [32] A multiyear study of the respiratory effects of long-term exposure to environmental tobacco smoke and air pollution reported that both long-term ozone and childhood exposure to maternal tobacco smoke were associated with diminished lung function in college students.[33] Viral infections also may contribute to susceptibility to COPD, and they are considered to play a role in the onset of airflow obstruction.
The direct costs of health care services and indirect costs through loss of productivity related to COPD amounted to $26 billion in 1998.26 About 14 million persons in the United States have COPD—about 12.5 million have chronic bronchitis and 1.9 million have emphysema.27 Emphysema has not increased, but since 1980, cases of chronic bronchitis increased 75 percent.27
Because national data systems will not be available in the first half of the decade for tracking progress, two subjects of interest concerning respiratory diseases are not addressed in this focus area’s objectives. The first topic addresses increasing the proportion of primary care providers who are trained to provide culturally competent health services to racial and ethnic groups seeking care for chronic obstructive pulmonary disease. The second involves increasing the proportion of primary care providers who are trained to use appropriate lung function tests to recognize the early signs of chronic obstructive pulmonary disease before the disease becomes serious and disabling.
Reliable statistics are not as available for COPD total cases, illness, disability, or death in African Americans, Hispanics, and other ethnic groups as for whites.[34], [35] From 1982 to 1984, the proportion of adults with COPD was 6.2 percent among whites and 3.2 percent among African Americans. In 1982, the age-adjusted COPD death rate for whites was 16.6 deaths per 1,000 population and 12.8 deaths per 1,000 for African Americans. Among the Hispanic groups studied, Puerto Ricans demonstrated a higher proportion of chronic bronchitis (2.9 percent) than Mexican Americans (1.7 percent) or Cuban Americans (1.7 percent).34, 35
In 1995, the proportion of the population with COPD was 5 percent in men aged 45 to 64 years and 11 percent in men aged 65 years and older. The proportion was 10 percent in women aged 45 to 64 years and 9 percent in women aged 65 to 74 years.
Death from COPD is more common in men than in women, and the death rate increases steeply with age.27, [36] Men and women have similar COPD death rates before age 55 years, but the rate for men rises thereafter. At age 70 years, the rate for men is more than double that for women, and at age 85 years and older, the COPD death rate for men is 3.5 times that for women.[37] The proportion was 8 percent for whites aged 45 to 64 years and 10 percent for whites aged 65 years and older. The proportion of African Americans with COPD was 6 percent for those aged 45 to 64 years and 8 percent for those aged 65 years and older.2 COPD death rates were lower in the Hispanic groups than in non-Hispanic whites; however, these rates have been increasing for Hispanics.33
Women might be more susceptible than men to developing COPD when exposed to risk factors such as tobacco smoke.[38] The beneficial effects of stopping smoking on the rate of lung function decline may be greater for women than men.[39]
Primary care physicians are in a key position to provide optimal care to patients with COPD and to provide counseling during clinical or health center visits to patients who smoke. Effective tests are available to screen patients for COPD, and primary care physicians need to be trained in the latest methods to detect and treat the disease.
Some 18 million persons in the United States were estimated to have OSA in 1993.[40] OSA affects all races, ages, and socioeconomic and ethnic groups.[41] Because OSA causes serious disturbances in normal sleep patterns, patients experience excessive daytime sleepiness and impaired performance. Common consequences of OSA range from personality changes and sexual dysfunction to falling asleep at work or while driving.40, 41
OSA symptoms include many repeated involuntary breathing pauses during sleep. The breathing pauses often are accompanied by choking sensations that may wake the patient. Other symptoms include intermittent snoring, awakening from sleep (poor sleep), early morning headaches, and excessive daytime sleepiness.
OSA can increase the seriousness of other lung diseases that decrease airflow, such as asthma and COPD. Cardiovascular deaths alone due to OSA have been estimated at 38,000 a year.40 Individuals with OSA often do not recognize reductions in alertness, diminished productivity, and discord in interpersonal relationships as part of the syndrome. Persons affected by OSA, for example, are seven times more likely to be involved in multiple vehicular crashes.[42] In children, OSA can disrupt sleep. OSA also may cause daytime behavioral problems that affect workplace performance and affect their learning ability in school.
Infants with siblings or parents who have OSA inherit an increased risk of sudden infant death syndrome (SIDS).[43] This tragic sleep-related breathing disorder takes the lives of more infants than all other causes combined.
OSA is prevalent particularly in men over age 50 years and in postmenopausal women, when hormonal changes appear to increase risk. The risk of OSA also is increased in certain racial and ethnic groups. Among young African Americans, the likelihood of experiencing OSA symptoms is twice that of young whites.[44] Nearly 50 percent of OSA patients have high blood pressure.[45], [46], [47]
A major factor in the pervasiveness of OSA’s effects on health and society has been the failure to educate people—and especially health care practitioners—about the disorder. A wide range of behavioral, mechanical, and surgical treatments can be used to manage OSA symptoms. Providing persons at risk with culturally and linguistically appropriate information about OSA could enable them to prevent or lessen the effects of OSA. Improved awareness of OSA symptoms represents a major public health challenge.
Primary care providers are an important barometer of OSA awareness because they are a first stop for patients who are seeking appropriate diagnosis and treatment. However, only 79 cases of sleep disorder were diagnosed in a sample of 10 million patient records from 1989 and 1990.40 In 1990 about a third of the medical schools in the United States offered no training in sleep medicine, and another third provided less than 2 hours on average for all sleep topics.[48] Data systems to track the training of health care providers in OSA over the decade are not currently available, and therefore the issue is not addressed in this focus area’s objectives. However, it represents an important research and data collection agenda. In the absence of strong educational models for physicians, the risk remains high that OSA will be misdiagnosed and mismanaged.
The National Commission on Sleep Disorders Research40 was established by the U.S. Congress in 1988 to assess the societal and economic impact of sleep disorders and the resources available to promote the prevention, diagnosis, and treatment of such disorders. In a 1994 report to Congress, the Commission concluded that even though the science of sleep disorders is not fully developed, such disorders can be prevented. The commission recommends that research on the natural history of sleep disorders be made an urgent national concern. Epidemiologic studies must be conducted to evaluate risk factors that lead to sleep disorders and to determine which sleep disorders lead to other serious health problems.
For the three objectives specific to asthma in Healthy People 2000, available data indicate movement away from the targets as the rate of hospitalizations and activity limitation increase and movement toward the target for increasing the proportion of persons with asthma who receive patient education. There were no objectives in Healthy People 2000 for COPD and OSA.
Note: Unless otherwise noted, data are from the Centers for Disease Control and Prevention, National Center for Health Statistics, Healthy People 2000 Review, 1998–99.
Respiratory Diseases
Goal: Promote respiratory health through better prevention, detection, treatment, and education efforts.
|
Number |
Objective Short Title |
|
Asthma |
|
|
24-1 |
Deaths from asthma |
|
24-2 |
Hospitalizations for asthma |
|
24-3 |
Hospital emergency department visits for asthma |
|
24-4 |
Activity limitations |
|
24-5 |
School or work days lost |
|
24-6 |
Patient education |
|
24-7 |
Appropriate asthma care |
|
24-8 |
Surveillance systems |
|
Chronic Obstructive Pulmonary Disease (COPD) |
|
|
24-9 |
Activity limitations due to chronic lung and breathing problems |
|
24-10 |
Deaths from COPD |
|
Obstructive Sleep Apnea (OSA) |
|
|
24-11 |
Medical evaluation and followup |
|
24-12 |
Vehicular crashes related to excessive sleepiness |
Reduce asthma deaths. |
Target and baseline:
|
Objective |
Age Group |
1998 Baseline |
2010 Target |
|
Rate per Million |
|||
|
24-1a. |
Children under age 5 years |
2.1 |
1.0 |
| 24-1b. |
Children aged 5 to 14 years |
3.3 |
1.0 |
|
24-1c. |
Adolescents and adults aged 15 to 34 years |
5.0 |
2.0 |
|
24-1d. |
Adults aged 35 to 64 years |
17.8 |
9.0 |
|
24-1e. |
Adults aged 65 years and older |
86.3 |
60.0 |
Target setting method: Better than the best.
Data source: National Vital Statistics System (NVSS), CDC, NCHS.
|
Select Age Groups, 1998 |
Asthma Deaths |
||||
|
24-1a. |
24-1b. |
24-1c. |
24-1d. |
24-1e. |
|
|
Rate per Million |
|||||
|
TOTAL |
2.1 |
3.3 |
5.0 |
17.8 |
86.3 |
|
Race and ethnicity |
|||||
|
American Indian or Alaska Native |
DSU |
DSU |
DSU |
DSU |
DSU |
|
Asian or Pacific Islander |
DSU |
DSU |
DSU |
12.8 |
136.9 |
|
Asian |
DNC |
DNC |
DNC |
DNC |
DNC |
|
Native Hawaiian |
DNC |
DNC |
DNC |
DNC |
DNC |
|
Black
or African |
8.1 |
9.7 |
16.6 |
52.3 |
130.4 |
|
White |
DSU |
2.0 |
3.0 |
13.3 |
81.1 |
|
|
|||||
|
Hispanic or Latino |
DSU |
DSU |
3.7 |
16.4 |
84.5 |
|
Not Hispanic or Latino |
2.1 |
3.5 |
6.9 |
17.8 |
86.2 |
|
Black or African American |
8.3 |
10.3 |
21.9 |
54.0 |
133.5 |
|
White |
DSU |
2.0 |
3.9 |
12.8 |
80.6 |
|
Gender |
|||||
|
Female |
1.4 |
2.7 |
4.3 |
22.3 |
99.1 |
|
Male |
2.8 |
4.0 |
5.7 |
13.0 |
68.1 |
|
Education (aged 25 to 64 years) |
|||||
|
Less than high school |
NA |
NA |
10.0* |
31.0 |
NA |
|
High school graduate |
NA |
NA |
11.4* |
22.9 |
NA |
|
At least some college |
NA |
NA |
3.9* |
9.3 |
NA |
DNA = Data have not been analyzed. DNC = Data are not
collected. DSU = Data are statistically unreliable. NA = Not applicable.
*Data are for persons aged 25 to 34 years.
24-2 | Reduce hospitalizations for asthma. |
Target and baseline:
|
Objective |
Age Group |
1998 Baseline |
2010 Target |
|
Rate per 10,000 |
|||
|
24-2a. |
Children under age 5 years |
45.6 |
25 |
|
24-2b. |
Children and adults aged 5 to 64 years* |
12.5 |
7.7 |
|
24-2c. |
Adults aged 65 years and older* |
17.7 |
11 |
*Age adjusted to the year 2000 standard population.
Target setting method: Better than the best.
Data source: National Hospital Discharge Survey (NHDS), CDC, NCHS.
|
Select Age Groups, 1998 |
Asthma Hospitalizations |
||
|
24-2a. |
24-2b. |
24-2c. |
|
|
Rate per 10,000 |
|||
|
TOTAL |
45.6 |
12.5 |
17.7 |
|
Race and ethnicity |
|||
|
American Indian or Alaska Native |
DSU |
DSU |
DSU |
|
Asian or Pacific Islander |
DSU |
DSU |
DSU |
|
Asian |
DNC |
DNC |
DNC |
|
Native Hawaiian and other Pacific Islander |
DNC |
DNC |
DNC |
|
Black or African American |
82.4 |
28.4 |
27.3 |
|
White |
29.5 |
7.8 |
12.4 |
|
|
|||
|
Hispanic or Latino |
DSU |
DSU |
DSU |
|
Not Hispanic or Latino |
DSU |
DSU |
DSU |
|
Black or African American |
DSU |
DSU |
DSU |
|
White |
DSU |
DSU |
DSU |
|
Gender |
|||
|
Female |
33.1 |
15.9 |
24.6 |
|
Male |
57.6 |
9.0 |
8.5 |
DNA = Data have not been analyzed. DNC = Data are not
collected. DSU = Data are statistically unreliable.
*Age adjusted to the year 2000 standard population.
Reduce hospital emergency department visits for asthma. |
Target and baseline:
|
Objective |
Age Group |
1995–97 Baseline |
2010 Target |
|
Rate per 10,000 |
|||
|
24-3a. |
Children under age 5 years |
150.0 |
80 |
|
24-3b. |
Children and adults aged 5 to 64 years |
71.1 |
50 |
|
24-3c. |
Adults aged 65 years and older |
29.5 |
15 |
Target setting method: Better than the best.
Data source: National Hospital Ambulatory Medical Care Survey (NHAMCS), CDC, NCHS.
|
Select Age Groups, 1995–97 |
Hospital Emergency
Department |
||
|
24-3a. |
24-3b. |
24-3c. |
|
|
Rate per 10,000 |
|||
|
TOTAL |
150.0 |
71.1 |
29.5 |
|
Race and ethnicity |
|||
|
American Indian or Alaska Native |
DSU |
DSU |
DSU |
|
Asian or Pacific Islander |
DSU |
DSU |
DSU |
|
Asian |
DNC |
DNC |
DNC |
|
Native Hawaiian and other Pacific Islander |
DNC |
DNC |
DNC |
|
Black or African American |
407.2 |
191.7 |
90.8 |
|
White |
101.7 |
53.4 |
23.1 |
|
|
|||
|
Hispanic or Latino |
DSU |
DSU |
DSU |
|
Not Hispanic or Latino |
DSU |
DSU |
DSU |
|
Black or African American |
DSU |
DSU |
DSU |
|
White |
DSU |
DSU |
DSU |
|
Gender |
|||
|
Female |
103.0 |
83.6 |
37.8 |
|
Male |
195.5 |
57.9 |
17.9 |
DNA = Data have not been analyzed. DNC = Data are not collected. DSU = Data are statistically unreliable.
Reduce activity limitations among persons with asthma. |
Target: 10 percent.
Baseline: 20 percent of persons with asthma experienced activity limitations in activity in 1994–96 (age adjusted to the year 2000 standard population).
Target setting method: Better than the best.
Data source: National Health Interview Survey (NHIS), CDC, NCHS.
|
Persons With Asthma, 1994–96 |
Experienced
|
|
Percent |
|
|
TOTAL |
20 |
|
Race and ethnicity |
|
|
American Indian or Alaska Native |
DSU |
|
Asian or Pacific Islander |
DSU |
|
Asian |
DSU |
|
Native Hawaiian and other Pacific Islander |
DSU |
|
Black or African American |
26 |
|
White |
18 |
|
|
|
|
Hispanic or Latino |
22 |
|
Not Hispanic or Latino |
19 |
|
Black or African American |
26 |
|
White |
18 |
|
Gender |
|
|
Female |
21 |
|
Male |
17 |
|
Family income level |
|
|
Poor |
28 |
|
Near poor |
20 |
|
Middle/high income |
16 |
DNA = Data have not been analyzed. DNC = Data are not
collected. DSU = Data are statistically unreliable.
Note: Age adjusted to the year 2000 standard population.
24-5 | (Developmental) Reduce the number of school or work days missed by persons with asthma due to asthma. |
Potential data source: National Health Interview Survey (NHIS), CDC, NCHS.
Increase the proportion of persons with asthma who receive formal patient education, including information about community and self-help resources, as an essential part of the management of their condition. |
Target: 30 percent.
Baseline: 8.4 percent of persons with asthma received formal patient education in 1998 (age adjusted to the year 2000 standard population).
Target setting method: Better than the best.
Data source: National Health Interview Survey (NHIS), CDC, NCHS.
|
Persons With Asthma, 1998 |
Received Patient Education |
|
Percent |
|
|
TOTAL |
8.4 |
|
Race and ethnicity |
|
|
American Indian or Alaska Native |
DSU |
|
Asian or Pacific Islander |
DSU |
|
Asian |
DSU |
|
Native Hawaiian and other Pacific Islander |
DSU |
|
Black or African American |
11.2 |
|
White |
7.8 |
|
|
|
|
Hispanic or Latino |
7.8 |
|
Not Hispanic or Latino |
8.4 |
|
Black or African American |
11.3 |
|
White |
7.9 |
|
Gender |
|
|
Female |
9.1 |
|
Male |
7.1 |
|
Family income level |
|
|
Poor |
7.2 |
|
Near poor |
10.3 |
|
Middle/high income |
8.4 |
DNA = Data have not been analyzed. DNC = Data are not
collected. DSU = Data are statistically unreliable.
Note: Age adjusted to the year 2000 standard population.
(Developmental) Increase the proportion of persons with asthma who receive appropriate asthma care according to the NAEPP Guidelines. |
24-7a. Persons with asthma who receive written asthma management plans from their health care provider.
24-7b. Persons with asthma with prescribed inhalers who receive instruction on how to use them properly.
24-7c. Persons with asthma who receive education about recognizing early signs and symptoms of asthma episodes and how to respond appropriately, including instruction on peak flow monitoring for those who use daily therapy.
24-7d. Persons with asthma who receive medication regimens that prevent the need for more than one canister of short-acting inhaled beta agonists per month for relief of symptoms.
24-7e. Persons with asthma who receive followup medical care for long-term management of asthma after any hospitalization due to asthma.
24-7f. Persons with asthma who receive assistance with assessing and reducing exposure to environmental risk factors in their home, school, and work environments.
Potential data source: National Health Interview Survey (NHIS), CDC, NCHS.
(Developmental) Establish in at least 25 States a surveillance system for tracking asthma death, illness, disability, impact of occupational and environmental factors on asthma, access to medical care, and asthma management. |
Potential data sources: Periodic surveys,Council of State and Territorial Epidemiologists and Public Health Foundation; Association of Schools of Public Health.
Reduce the proportion of adults whose activity is limited due to chronic lung and breathing problems. |
Target: 1.5 percent.
Baseline: 2.2 percent of adults aged 45 years and older experienced activity limitations due to chronic lung and breathing problems in 1997 (age adjusted to the year 2000 standard population).
Target setting method: Better than the best.
Data source: National Health Interview Survey (NHIS), CDC, NCHS.
|
Adults Aged 45 Years and Older, 1997 |
Experienced
|
|
Percent |
|
|
TOTAL |
2.2 |
|
Race and ethnicity |
|
|
American Indian or Alaska Native |
DSU |
|
Asian or Pacific Islander |
DSU |
|
Asian |
DSU |
|
Native Hawaiian and other Pacific Islander |
DSU |
|
Black or African American |
2.3 |
|
White |
2.3 |
|
|
|
|
Hispanic or Latino |
1.7 |
|
Not Hispanic or Latino |
2.3 |
|
Black or African American |
2.2 |
|
White |
2.3 |
|
Gender |
|
|
Female |
2.1 |
|
Aged 45 to 64 years |
1.6 |
|
Aged 65 years and older |
3.0 |
|
Male |
2.5 |
|
Aged 45 to 64 years |
1.6 |
|
Aged 65 years and older |
4.1 |
|
Family income level |
|
|
Poor |
5.2 |
|
Near poor |
4.0 |
|
Middle/high income |
1.8 |
DNA = Data have not been analyzed. DNC = Data are not
collected. DSU = Data are statistically unreliable.
Note: Age adjusted to the year 2000 standard population.
Reduce deaths from chronic obstructive pulmonary disease (COPD) among adults. |
Target: 60 deaths per 100,000 adults.
Baseline: 119.4 deaths from COPD per 100,000 persons aged 45 years and older occurred in 1998 (age adjusted to the year 2000 standard population).
Target setting method: 50 percent improvement.
Data source: National Vital Statistics System (NVSS), CDC, NCHS.
|
Adults Aged 45 Years and Older, 1998 |
Chronic |
|
Rate per 100,000 |
|
|
TOTAL |
119.4 |
|
Race and ethnicity |
|
|
American Indian or Alaska Native |
79.6 |
|
Asian or Pacific Islander |
48.6 |
|
Asian |
DNC |
|
Native Hawaiian and other Pacific Islander |
DNC |
|
Black or African American |
85.3 |
|
White |
124.3 |
|
|
|
|
Hispanic or Latino |
52.5 |
|
Not Hispanic or Latino |
122.8 |
|
Black or African American |
87.2 |
|
White |
127.9 |
|
Gender |
|
|
Female |
98.8 |
|
Male |
153.7 |
|
Education (aged 25 to 64 years) |
|
|
Less than high school |
19.7 |
|
High school graduate |
12.5 |
|
At least some college |
4.4 |
DNA = Data have not been analyzed. DNC = Data are not
collected. DSU = Data are statistically unreliable.
Note: Age adjusted to the year 2000 standard population.
(Developmental) Increase the proportion of persons with symptoms of obstructive sleep apnea whose condition is medically managed. |
24-11a. Persons with excessive daytime sleepiness, loud snoring, and other signs associated with obstructive sleep apnea who seek medical evaluation.
24-11b. Persons with excessive daytime sleepiness, loud snoring, and other signs associated with obstructive sleep apnea who receive followup medical care for long-term management of their condition.
Potential data source: National Health Interview Survey (NHIS), CDC, NCHS.
(Developmental) Reduce the proportion of vehicular crashes caused by persons with excessive sleepiness. |
Potential data source: National Health Interview Survey (NHIS), CDC, NCHS. Fatality Analysis Reporting System (FARS), U.S. Department of Transportation, National Highway Traffic Safety Administration.
(A listing of abbreviations and acronyms used in this publication appears in Appendix H.)
Ambulatory care: Medical care provided at hospital emergency and outpatient departments.
Asthma: A lung disease characterized by airway constriction, mucus secretion, and chronic inflammation, resulting in reduced airflow and wheezing, coughing, chest tightness, and difficulty breathing.
Chronic bronchitis: A lung disease characterized by the presence of chronic productive cough most days for 3 months in each of 2 successive years.
Chronic obstructive pulmonary disease (COPD): A lung disease characterized by airflow obstruction due to chronic bronchitis and emphysema, two diseases that often occur together. COPD is one of the most common respiratory conditions among adults worldwide and is the fourth leading cause of death in the United States.
Dyspnea: Shortness of breath.
Emphysema: Abnormal permanent enlargement of the airspaces in the lungs accompanied by coughing and difficulty breathing.
Epidemiologic studies: Studies of disease occurrence.
Obstructive sleep apnea (OSA): An illness characterized by snoring, partial or complete cessation of breathing during sleep, reductions in blood oxygen levels, severe sleep disruptions, and excessive daytime sleepiness. OSA is a chronic breathing problem with serious effects on individual health and productivity, including an inheritable risk of sudden infant deaths, behavior and learning disturbances, injury from accidents, and reduced quality of life.
Rate: The basic measure of disease occurrence that most clearly expresses the probability of risk of disease in a defined population over a specified period of time. A rate is defined as:
Number of
events
Population at risk
[1] Mannino, D.M.; Homa, D.M.; Pertowski, C.A.; et al. Surveillance for asthma—United States, 1960–1995. Morbidity and Mortality Weekly ReportCDC Surveillance Summaries 47(1):1-27, 1998. PubMed; PMID 9580746
[2] Benson, V., and Marano, M.A. Current estimates from the National Health Interview Survey, 1995. Vital and Health Statistics 10(199):1-428, 1998. PubMed; PMID 9914773
[3] National Heart, Lung, and Blood Institute (NHLBI). Data Fact Sheet. Asthma Statistics. Bethesda, MD: National Institutes of Health (NIH), Public Health Service (PHS), 1999.
[4] National Center for Health Statistics (NCHS). Current estimates from the National Health Interview Survey, 1990. Vital and Health Statistics 10(194), 1997.
[5] National Asthma Education and Prevention Program. Expert Panel Report 2: Guidelines for the Diagnosis and Management of Asthma. NIH Pub. No. 97-4051. Bethesda, MD: NIH, 1997.
[6] NCHS. Ambulatory care visits to physicians’ offices, hospital outpatient departments, and emergency departments: United States, 1996. Vital and Health Statistics 13(134), 1998. PubMed; PMID 9564280
[7] NCHS. Healthy People 2000 Review, 1998–99.Hyattsville, MD: PHS, 1999.
[8] Weiss, K.B.; Gergen, P.J.; and Hodgson, T.A. An economic evaluation of asthma in the United States. New England Journal of Medicine 326:862-866, 1992. PubMed; PMID 1542323
[9] Sullivan, S.; Elixhauser, S.; Buist, A.S.; et al. National Asthma Education and Prevention Program working group report on the cost effectiveness of asthma care. American Journal of Respiratory and Critical Care Medicine 154(3, Part 2):584-595, 1996. PubMed; PMID 8810630
[10] Glaxco Canada. The Costs of Asthma in Canada. Princeton, NJ: Communications Media for Education, 1993.
[11] Koren, H.S. Environmental risk factors in atopic asthma. International Archives of Allergy and Immunology 113:65-68, 1997. PubMed; PMID 9130486
[12] Becklake, M.R., and Ernst, P. Environmental factors. Lancet 350(Suppl. 2):10-13, 1997. PubMed; PMID 9343098
[13] Office of Air Quality Planning and Standards, U.S. Environmental Protection Agency (EPA). National Air Quality and Emissions Report, 1997. CPA Pub. No. EPA 454/R-98-016. Research Triangle Park, NC: EPA, 1998.
[14] Schwartz, D.A., and Peterson, M.W. Occupational lung disease. Advances in Internal Medicine 42:269-312, 1997. PubMed; PMID 9048122
[15] Busse, W.W.; Gern, J.E.; and Dick, E.C. The role of respiratory viruses in asthma. Ciba Foundation Symposium 206:208-213, 1997. PubMed; PMID 9257014
[16] U.S. Department of Health and Human Services (HHS). Action Against Asthma: A Strategic Plan for the Department of Health and Human Services. Washington, DC: HHS, 2000.
[17] Wade, S.; Weil, C.; Holden, G.; et al. Psycho social characteristics of inner-city children with asthma: A description of the NCICAS psychosocial protocol. National Cooperative Inner-City Asthma Study. Pediatric Pulmonology 24:263-276, 1997. PubMed; PMID 9368260
[18] Evans, D.; Mellins, R.; Lobach, K.; et al. Improving care for minority children with asthma: Professional education in public health clinics. Pediatrics 99:157-164, 1997. PubMed; PMID 9024439
[19] Institute of Medicine. Cleaning the Air: Asthma and Indoor Air Exposures. Washington, DC: National Academy Press, 2000.
[20] NHLBI. National Asthma Education and Prevention Program Summary Report. Bethesda, MD: NIH, 1999.
[21] NCHS. Health, United States, 1986.Hyattsville, MD: NCHS, 1986.
[22] NCHS. Health, United States, 1999 withHealth and Aging Chartbook. Hyattsville, MD: NCHS, 1999.
[23] Bone, R.C.; Dantzker, D.R.; and George, R.B. Pulmonary and Critical Care Medicine. St. Louis, MO: Mosby Year Book, 1993, Chapter G-1.
[24] Sherril, D.L.; Lebowitz, M.D.; and Burrows, B. Epidemiology of COPD. Clinical Chest Medicine 11:375-388, 1990. PubMed; PMID 2205437
[25] Fletcher, C., and Peto, R. The natural history of COPD. British Medical Journal 1:1645-1648, 1977. PubMed; PMID 871704
[26] Fishman, A.P. Pulmonary Diseases and Disorders. 2nd ed. New York, NY: McGraw-Hill, Inc., 1998.
[27] NHLBI. Morbidity and Mortality: 1998 Chartbook on Cardiovascular, Lung and Blood Diseases. Bethesda, MD: NIH, 1998.
[28] Schwartz, D.A., and Peterson, M.W. Occupational lung disease. Disease-A-Month 44:41-84, 1998. PubMed; PMID 9487302
[29] Wynder, E.L., and Hoffmann, D. Tobacco and health: A societal challenge. New England Journal of Medicine 300:894-903, 1979. PubMed; PMID 370598
[30] Bakke, S.; Baste, V.; Hanoa, R.; et al. Prevalence of obstructive lung disease in a general population: Relation to occupational title and exposure to some airborne agents. Thorax 46(12):863-870, 1991. PubMed; PMID 1792631
[31] Souza, M.B.; Saldiva, P.H.; Pope, III, C.A.; et al. Respiratory changes due to long-term exposure to urban levels of air pollution: A histopathologic study in humans. Chest 113:1312-1318, 1998. PubMed; PMID 9596312
[32] Dockery, D.W., and Brunekreef, B. Longitudinal studies of air pollution effects on lung function. American Journal of Respiratory and Critical Care Medicine 154(6, Part 2):S250-S256, 1996. PubMed; PMID 8970397
[33] Galizia, A., and Kinney, P.L. Long-term residence in areas of high ozone: Associations with respiratory health in a nationwide sample of nonsmoking young adults. Environmental Health Perspectives 107(8):675-679, 1999. PubMed; PMID 10417367
[34] Coultas, D.B.; Gong, Jr., H.; Grad, R.; et al. Respiratory diseases in minorities of the United States. American Journal of Respiratory and Critical Care Medicine 149:S93-S131, 1993. PubMed; PMID 8118656
[35] Gibson, K.F.; Aguayo, S.M.; Flowers, J.C.; et al. NHLBI special report. Respiratory diseases disproportionately affecting minorities. Chest 108:1380-1392, 1995. PubMed; PMID 7587446
[36] Higgins, M.W., and Keller, J.B. Trends in COPD morbidity and mortality in Tecumseh, Michigan. Annual Review of Respiratory Diseases 140:S42-S48, 1989. PubMed; PMID 2782759
[37] Feinlieb, M.; Rosenburg, H.M.; Collins, J.G.; et al. Trends in COPD morbidity and mortality in the United States. American Journal of Respiratory Diseases 140:S9-S18, 1989. PubMed; PMID 2782766
[38] Tashkin, D.P.; Altose, M.F.; Bleecker, E.R.; et al. The Lung Health Study: Airway responsiveness to inhaled methacholine in smokers with mild to moderate airflow limitation. American Review of Respiratory Diseases 145:301-310, 1992. PubMed; PMID 1736734
[39] Anthonisen, N.R.; Connell, J.E.; Kiley, J.P.; et al. Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1: The Lung Health Study. Journal of the American Medical Association 272:1497-1505, 1994. PubMed; PMID 7966841
[40] National Institute on Aging (NIA). Wake Up America: A National Sleep Alert, Report of the National Commission on Sleep Disorders Research to the U.S. Congress and Department of Health and Human Services. Bethesda, MD: NIA, 1994.
[41] Redline, S., and Strohl, K.P. Recognition and consequences of obstructive sleep apnea hypopnea syndrome. Clinical Chest Medicine 19:1-19, 1998. PubMed; PMID 9554214
[42] Young, T.; Blustein, J.; Finn, L.; et al. Sleep-disordered breathing and motor vehicle accidents in a population-based sample of employed adults. Sleep 20:608-613, 1997. PubMed; PMID 9351127
[43] Tischler, P.V.; Redline, S.; Ferrette, V.; et al. The association of sudden unexpected infant death with obstructive sleep apnea. American Journal of Respiratory and Critical Care Medicine 153:1857-1863, 1996. PubMed; PMID 8665046
[44] Redline, S. Epidemiology of sleep disordered breathing. Seminars in Respiratory and Critical Care Medicine 19(2):113-122.
[45] Fletcher, E.C.; DeBehunke, R.D.; Lovoi, M.S.; et al. Undiagnosed sleep apnea in patients with essential hypertension. Annals of Internal Medicine 103:190-195, 1995. PubMed; PMID 4014900
[46] Guilleminault, H.C.; Tilkian, A.; and Dement, W.C. The sleep apnea syndromes. Annual Review of Medicine 27:465-484, 1976. PubMed; PMID 180875
[47] Carlson, J.T.; Hedner, J.A.; Ejnell, H.; et al. High prevalence of hypertension in sleep apnea patients independent of obesity. American Journal of Respiratory and Critical Care Medicine 150:72-77, 1994. PubMed; PMID 8025776
[48] Rosen, R.C.; Rosekind, M.; Rosevear, C.; et al. Physician education in sleep and sleep disorders: A national survey of U.S. medical schools. Sleep 16:249-254, 1993. PubMed; PMID 8506458