
|
| May 27, 2010 |
|
During 2008, an estimated 3,224,014 drug-related ED visits were made by patients aged 25 or older, of which 4.3 percent (138,108 visits) involved a suicide attempt. Many of the ED visits for drug-related suicide attempts involved multiple drugs, with an overall average of 2.4 drugs per ED visit for both males and females. More than half (57.7 percent) of the ED visits for drug-related suicide attempts were made by females.
Almost two thirds of the ED visits for drug-related suicide attempts by adults aged 25 or older were made by patients in the 25 to 34 and 35 to 44 age groups (31.8 and 30.9 percent, respectively), and one quarter of the visits were made by patients aged 45 to 54 (24.6 percent) (Figure 1). About one in eight visits (12.6 percent) were made by patients aged 55 or older.

|
| Age Group | Percent |
|---|---|
| 25 to 34 | 31.8% |
| 35 to 44 | 30.9% |
| 45 to 54 | 24.6% |
| 55 to 64 | 9.4% |
| 65 or Older | 3.2% |
| Source: 2008 (08/2009 update) SAMHSA Drug Abuse Warning Network (DAWN). |
Pharmaceuticals were involved in 94.9 percent of ED visits for drug-related suicide attempts among adults aged 25 or older (Table 1). Alcohol in combination with other drugs was involved in one third (32.8 percent) of all visits. Illicit drugs were involved in about one fifth (19.1 percent) of these visits, with 12.3 percent involving cocaine and 7.2 percent involving marijuana.8
| Drug Category | Estimated Number of ED Visits** |
Percent of Visits** |
|---|---|---|
| Total ED Visits | 138,108 | 100.0% |
| Alcohol Combined with Other Drugs | 45,300 | 32.8% |
| Illicit Drugs | 26,337 | 19.1% |
| Cocaine | 17,032 | 12.3% |
| Marijuana | 9,999 | 7.2% |
| Pharmaceuticals | 131,106 | 94.9% |
| Anti-anxiety Drugs (e.g., Anxiolytics, Sedatives, and Hypnotics) | 62,522 | 45.3% |
| Benzodiazepines (e.g., Alprazolam) | 46,472 | 33.6% |
| Antidepressants | 28,972 | 21.0% |
| Antipsychotics (e.g., Quetiapine) | 18,844 | 13.6% |
| Narcotic Painkillers (e.g., Oxycodone) | 21,302 | 15.4% |
| Acetaminophen Products | 14,775 | 10.7% |
| Anticonvulsants | 10,348 | 7.5% |
| Cardiovascular Agents | 11,024 | 8.0% |
| * Other drugs involved in suicide attempts were typically found at levels of less than 5 percent, and often less than 1 percent; therefore, data are not shown. ** Because multiple drugs may be involved in each visit, estimates of visits by drug may add to more than the total, and percentages may add to more than 100 percent. Source: 2008 (08/2009 update) SAMHSA Drug Abuse Warning Network (DAWN). |
Anti-anxiety drugs were involved in 45.3 percent of ED visits for drug-related suicide attempts, the majority of which could be attributed to benzodiazepines (33.6 percent). Antidepressants were involved in 21.0 percent of these visits, while antipsychotics accounted for 13.6 percent. Narcotic painkillers accounted for 15.4 percent of such visits, while pain medications containing acetaminophen as their main ingredient were involved in 10.7 percent, and anticonvulsants accounted for 7.5 percent of these ED visits. Cardiovascular agents were involved in 8.0 percent of these ED visits. Other prescription and over-the-counter (OTC) pharmaceuticals, including gastrointestinal agents (e.g., laxatives) and respiratory agents (e.g., antihistamines), involved in ED visits for drug-related suicide attempts among adults aged 25 or older were typically found at rates of less than 5 percent (data not shown).
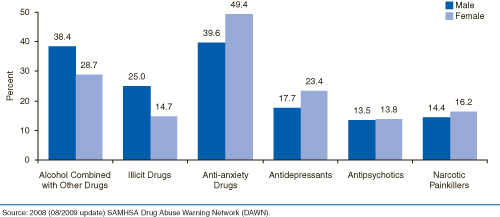
The drugs involved in ED visits for drug-related suicide attempts varied by gender. Anti-anxiety drugs were more likely to be involved in visits made by females than those made by males (49.4 vs. 39.6 percent), as were antidepressants (23.4 vs. 17.7 percent) (Figure 2). Conversely, ED visits involving drug-related suicide attempts by males were more likely than those by females to involve alcohol in combination with other drugs (38.4 vs. 28.7 percent) and illicit drugs (25.0 vs. 14.7 percent). Antipsychotics and narcotic painkillers each were involved in more than 1 in 10 ED visits made by males (13.5 and 14.4 percent, respectively) and females (13.8 and 16.2 percent, respectively).
|
| Gender | Alcohol Combined with Other Drugs |
Illicit Drugs | Anti-anxiety Drugs |
Antidepressants | Antipsychotics | Narcotic Painkillers |
|---|---|---|---|---|---|---|
| Male | 38.4% | 25.0% | 39.6% | 17.7% | 13.5% | 14.4% |
| Female | 28.7% | 14.7% | 49.4% | 23.4% | 13.8% | 16.2% |
| Source: 2008 (08/2009 update) SAMHSA Drug Abuse Warning Network (DAWN). |
The drugs involved in ED visits for drug-related suicide attempts also varied by age group (Table 2). Anti-anxiety drugs accounted for the largest proportions of substances involved with these visits across all age groups (ranging from 41.7 to 62.0 percent). Anti-anxiety drugs were involved in approximately 6 in 10 of such visits among patients aged 55 to 64 and 65 or older (58.4 and 62.0 percent, respectively). Of these, benzodiazepines were involved in more than one third (37.3 percent) of such visits made by patients aged 55 to 64 and in more than half (50.7 percent) made by patients aged 65 or older. About one third of visits among patients in the 25 to 34, 35 to 44, and 45 to 54 age groups involved alcohol in combination with other drugs (31.8, 36.4, and 34.0 percent, respectively), compared with about one quarter (25.9 percent) of visits among patients aged 55 to 64 and about one fifth (19.9 percent) of those for patients aged 65 or older. Nearly one quarter (24.2 percent) of visits among patients aged 35 to 44 involved illicit drugs, with smaller percentages for other age groups. Antipsychotic drugs accounted for more than one in five visits among patients aged 65 or older (21.5 percent). Smaller percentages of visits involved narcotic painkillers (e.g., hydrocodone and oxycodone products), ranging from 13.2 percent among patients aged 65 or older to 16.9 percent among patients aged 55 to 64.
| Drug Category | Percent Aged 25 to 34 |
Percent Aged 35 to 44 |
Percent Aged 45 to 54 |
Percent Aged 55 to 64 |
Percent Aged 65 or Older |
|---|---|---|---|---|---|
| Alcohol Combined with Other Drugs | 31.8% | 36.4% | 34.0% | 25.9% | 19.9% |
| Illicit Drugs | 21.7% | 24.2% | 16.0% | 7.6% | * |
| Anti-anxiety Drugs | 42.7% | 41.7% | 45.9% | 58.4% | 62.0% |
| Benzodiazepines | 30.6% | 31.1% | 37.1% | 37.3% | 50.7% |
| Antidepressants | 21.9% | 19.3% | 23.9% | 14.5% | 24.3% |
| Antipsychotics | 16.1% | 10.8% | 15.5% | 7.0% | 21.5% |
| Narcotic Painkillers | 16.3% | 15.6% | 13.8% | 16.9% | 13.2% |
| Hydrocodone Products | 5.5% | 8.9% | 5.3% | 7.1% | 7.3% |
| Oxycodone Products | 5.3% | 4.2% | 4.6% | 6.2% | 1.5% |
| * The percentage of illicit drugs among ED visits by adults aged 65 or older was suppressed because of small sample size. Source: 2008 (08/2009 update) SAMHSA Drug Abuse Warning Network (DAWN). |
While suicide prevention efforts have historically targeted youths, young adults, and elderly men, the findings in this report suggest that adults aged 25 to 54 may also be appropriate targets for drug-related suicide prevention campaigns. The patterns of drug involvement for persons of different ages and genders suggest that interventions might be most effective if they are tailored to match the behaviors and needs of specific groups. Moreover, given the high involvement of prescription drugs in ED visits for drug-related suicide attempts made by patients aged 25 or older, doctors and families need to be educated about the potential use of prescription drugs as a method of or influence on suicide attempts.
| The Drug Abuse Warning Network (DAWN) is a public health surveillance system that monitors drug-related morbidity and mortality. DAWN uses a probability sample of hospitals to produce estimates of drug-related emergency department (ED) visits for the United States and selected metropolitan areas annually. DAWN also produces annual profiles of drug-related deaths reviewed by medical examiners or coroners in selected metropolitan areas and States. Any ED visit related to recent drug use is included in DAWN. All types of drugs—licit and illicit—are covered. Alcohol is included for adults when it occurs with another drug. Alcohol is always reported for minors even if no other drug is present. DAWN's method of classifying drugs was derived from the Multum Lexicon, Copyright 2008, Multum Information Services, Inc. The Multum Licensing Agreement can be found in DAWN annual publications at http://www.multum.com/license.htm. DAWN is one of three major surveys conducted by the Substance Abuse and Mental Health Services Administration's Office of Applied Studies (SAMHSA/OAS). For more information on other OAS surveys, go to http://www.oas.samhsa.gov/. SAMHSA has contracts with Westat (Rockville, MD) and RTI International (Research Triangle Park, NC) to operate the DAWN system and produce publications. For publications and additional information about DAWN, go to http://DAWNinfo.samhsa.gov/. |
| The DAWN Report is published periodically by the Office of Applied Studies, Substance Abuse and Mental Health Services Administration (SAMHSA). All material appearing in this report is in the public domain and may be reproduced or copied without permission from SAMHSA. Additional copies of this report or other reports from the Office of Applied Studies are available online: http://samhsa.gov/data/. Citation of the source is appreciated. For questions about this report, please e-mail: shortreports@samhsa.hhs.gov.
DAWN_003 |
This page was last updated on September 29, 2009. |