General Information About Breast Cancer
Stages of Breast Cancer
Inflammatory Breast Cancer
Recurrent Breast Cancer
Treatment Option Overview
Treatment Options by Stage
Treatment Options for Inflammatory Breast Cancer
Treatment Options for Triple-Negative Breast Cancer
Treatment Options for Recurrent Breast Cancer
To Learn More About Breast Cancer
Changes to This Summary (10/03/2012)
Get More Information From NCI
About PDQ
General Information About Breast Cancer
Key Points for This Section
- Breast cancer is a disease in which malignant (cancer) cells form in the tissues of the breast.
- Age and health history can affect the risk of developing breast cancer.
- Breast cancer is sometimes caused by inherited gene mutations (changes).
- Possible signs of breast cancer include a lump or change in the breast.
- Tests that examine the breasts are used to detect (find) and diagnose breast cancer.
- If cancer is found, tests are done to study the cancer cells.
- Certain factors affect prognosis (chance of recovery) and treatment options.
Breast cancer is a disease in which malignant (cancer) cells form in the tissues of the breast.
The breast is made up of lobes and ducts. Each breast has 15 to 20 sections called lobes, which have many smaller sections called lobules. Lobules end in dozens of tiny bulbs that can make milk. The lobes, lobules, and bulbs are linked by thin tubes called ducts.
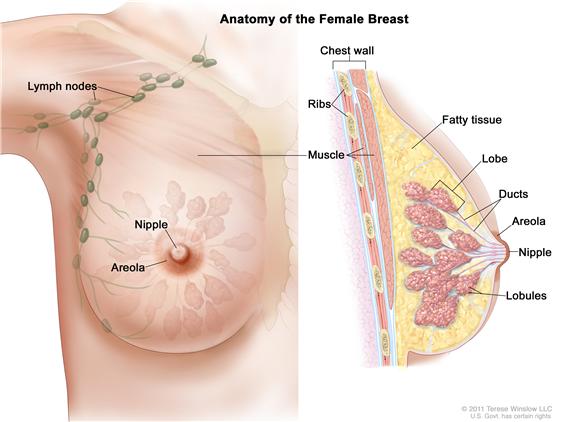
Each breast also has blood vessels and lymph vessels. The lymph vessels carry an almost colorless fluid called lymph. Lymph vessels lead to organs called lymph nodes. Lymph nodes are small bean-shaped structures that are found throughout the body. They filter substances in a fluid called lymph and help fight infection and disease. Clusters of lymph nodes are found near the breast in the axilla (under the arm), above the collarbone, and in the chest.
The most common type of breast cancer is ductal carcinoma, which begins in the cells of the ducts. Cancer that begins in the lobes or lobules is called lobular carcinoma and is more often found in both breasts than are other types of breast cancer. Inflammatory breast cancer is an uncommon type of breast cancer in which the breast is warm, red, and swollen.
See the PDQ summary on Unusual Cancers of Childhood for information about childhood breast cancer.
Age and health history can affect the risk of developing breast cancer.
Anything that increases your chance of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn't mean that you will not get cancer. Talk with your doctor if you think you may be at risk. Risk factors for breast cancer include the following:
- Older age.
- Menstruating at an early age.
- Older age at first birth or never having given birth.
- A personal history of breast cancer or benign (noncancer) breast disease.
- A mother or sister with breast cancer.
- Treatment with radiation therapy to the breast/chest.
- Breast tissue that is dense on a mammogram.
- Taking hormones such as estrogen and progesterone.
- Drinking alcoholic beverages.
- Being white.
NCI's Breast Cancer Risk Assessment Tool uses a woman's risk factors to estimate her risk for breast cancer during the next five years and up to age 90. This online tool is meant to be used by a health care provider. For more information on breast cancer risk, call 1-800-4-CANCER.
Breast cancer is sometimes caused by inherited gene mutations (changes).
The genes in cells carry the hereditary information that is received from a person’s parents. Hereditary breast cancer makes up about 5% to 10% of all breast cancer. Some mutated genes related to breast cancer are more common in certain ethnic groups.
Women who have a mutated gene related to breast cancer and who have had breast cancer in one breast have an increased risk of developing breast cancer in the other breast. These women also have an increased risk of ovarian cancer, and may have an increased risk of other cancers. Men who have a mutated gene related to breast cancer also have an increased risk of this disease. For more information, see the PDQ summary on Male Breast Cancer Treatment.
There are tests that can detect (find) mutated genes. These genetic tests are sometimes done for members of families with a high risk of cancer. See the following PDQ summaries for more information:
Possible signs of breast cancer include a lump or change in the breast.
Breast cancer may cause any of the following signs and symptoms. Check with your doctor if you have any of the following problems:
- A lump or thickening in or near the breast or in the underarm area.
- A change in the size or shape of the breast.
- A dimple or puckering in the skin of the breast.
- A nipple turned inward into the breast.
- Fluid, other than breast milk, from the nipple, especially if it's bloody.
- Scaly, red, or swollen skin on the breast, nipple, or areola (the dark area of skin that is around the nipple).
- Dimples in the breast that look like the skin of an orange, called peau d’orange.
Other conditions that are not breast cancer may cause these same symptoms.
Tests that examine the breasts are used to detect (find) and diagnose breast cancer.
A doctor should be seen if changes in the breast are noticed. The following tests and procedures may be used:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Clinical breast exam (CBE): An exam of the breast by a doctor or other health professional. The doctor will carefully feel the breasts and under the arms for lumps or anything else that seems unusual.
- Mammogram: An x-ray of the breast.
- Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. The picture can be printed to be looked at later.
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease in the organ or tissue that makes it.
- Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. If a lump in the breast is found, the doctor may need to remove a small piece of the lump. Four types of biopsies are as follows:
- Excisional biopsy: The removal of an entire lump of tissue.
- Incisional biopsy: The removal of part of a lump or a sample of tissue.
- Core biopsy: The removal of tissue using a wide needle.
- Fine-needle aspiration (FNA) biopsy: The removal of tissue or fluid, using a thin needle.

If cancer is found, tests are done to study the cancer cells.
Decisions about the best treatment are based on the results of these tests. The tests give information about:
- how quickly the cancer may grow.
- how likely it is that the cancer will spread through the body.
- how well certain treatments might work.
- how likely the cancer is to recur (come back).
Tests include the following:
- Estrogen and progesterone receptor test: A test to measure the amount of estrogen and progesterone (hormones) receptors in cancer tissue. If there are more estrogen and progesterone receptors than normal, the cancer may grow more quickly. The test results show whether treatment to block estrogen and progesterone may stop the cancer from growing.
- Human epidermal growth factor type 2 receptor (HER2/neu) test: A laboratory test to measure how many HER2/neu genes there are and how much HER2/neu protein is made in a sample of tissue. If there are more HER2/neu genes or higher levels of HER2/neu protein than normal, the cancer may grow more quickly and is more likely to spread to other parts of the body. The cancer may be treated with drugs that target the HER2/neu protein, such as trastuzumab and lapatinib.
- Multigene tests: Tests in which samples of tissue are studied to look at the activity of many genes at the same time. These tests may help predict whether cancer will spread to other parts of the body or recur (come back).
- Oncotype DX: This test helps predict whether stage I or stage II breast cancer that is estrogen receptor positive and node-negative will spread to other parts of the body. If the risk of the cancer spreading is high, chemotherapy may be given to lower the risk.
- MammaPrint: This test helps predict whether stage I or stage II breast cancer that is node-negative will spread to other parts of the body. If the risk of the cancer spreading is high, chemotherapy may be given to lower the risk.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) and treatment options depend on the following:
- The stage of the cancer (the size of the tumor and whether it is in the breast only or has spread to lymph nodes or other places in the body).
- The type of breast cancer.
- Estrogen receptor and progesterone receptor levels in the tumor tissue.
- Human epidermal growth factor type 2 receptor (HER2/neu) levels in the tumor tissue.
- Whether the tumor tissue is triple-negative (cells that do not have estrogen receptors, progesterone receptors, or high levels of HER2/neu).
- How fast the tumor is growing.
- How likely the tumor is to recur (come back).
- A woman’s age, general health, and menopausal status (whether a woman is still having menstrual periods).
- Whether the cancer has just been diagnosed or has recurred (come back).
Stages of Breast Cancer
Key Points for This Section
After breast cancer has been diagnosed, tests are done to find out if cancer cells have spread within the breast or to other parts of the body.
The process used to find out whether the cancer has spread within the breast or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment. The following tests and procedures may be used in the staging process:
- Sentinel lymph node biopsy: The removal of the sentinel lymph node during surgery. The sentinel lymph node is the first lymph node to receive lymphatic drainage from a tumor. It is the first lymph node the cancer is likely to spread to from the tumor. A radioactive substance and/or blue dye is injected near the tumor. The substance or dye flows through the lymph ducts to the lymph nodes. The first lymph node to receive the substance or dye is removed. A pathologist views the tissue under a microscope to look for cancer cells. If cancer cells are not found, it may not be necessary to remove more lymph nodes.
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- Bone scan: A procedure to check if there are rapidly dividing cells, such as cancer cells, in the bone. A very small amount of radioactive material is injected into a vein and travels through the bloodstream. The radioactive material collects in the bones and is detected by a scanner.
- PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
There are three ways that cancer spreads in the body.
The three ways that cancer spreads in the body are:
- Through tissue. Cancer invades the surrounding normal tissue.
- Through the lymph system. Cancer invades the lymph system and travels through the lymph vessels to other places in the body.
- Through the blood. Cancer invades the veins and capillaries and travels through the blood to other places in the body.
When cancer cells break away from the primary (original) tumor and travel through the lymph or blood to other places in the body, another (secondary) tumor may form. This process is called metastasis. The secondary (metastatic) tumor is the same type of cancer as the primary tumor. For example, if breast cancer spreads to the bones, the cancer cells in the bones are actually breast cancer cells. The disease is metastatic breast cancer, not bone cancer.
The following stages are used for breast cancer:
This section describes the stages of breast cancer. The breast cancer stage is based on the results of testing that is done on the tumor and lymph nodes removed during surgery and other tests.
There are 3 types of breast carcinoma in situ:
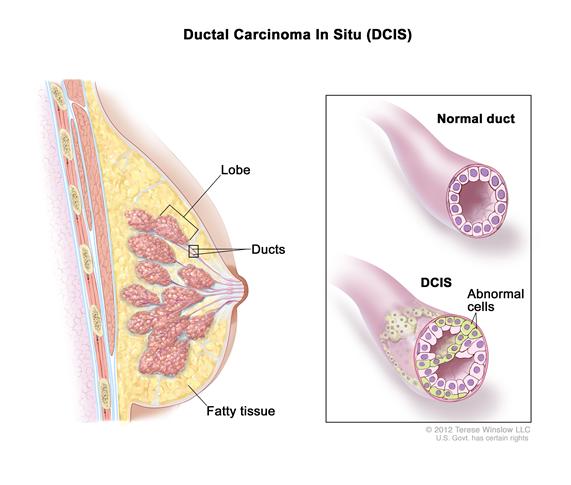
- Ductal carcinoma in situ (DCIS) is a noninvasive condition in which abnormal cells are found in the lining of a breast duct. The abnormal cells have not spread outside the duct to other tissues in the breast. In some cases, DCIS may become invasive cancer and spread to other tissues. At this time, there is no way to know which lesions could become invasive.
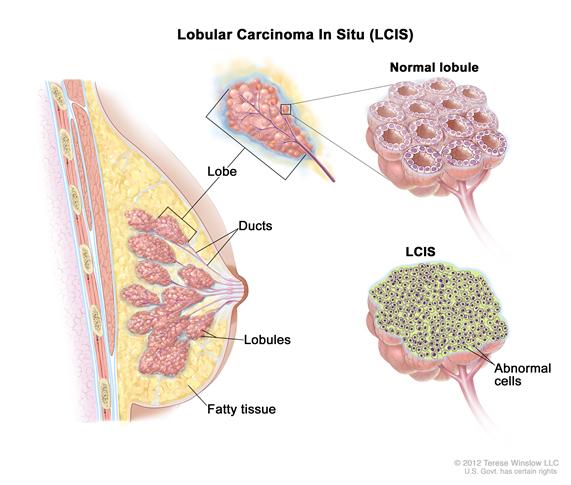
- Lobular carcinoma in situ (LCIS) is a condition in which abnormal cells are found in the lobules of the breast. This condition seldom becomes invasive cancer. However, having LCIS in one breast increases the risk of developing breast cancer in either breast.
- Paget disease of the nipple is a condition in which abnormal cells are found in the nipple only.
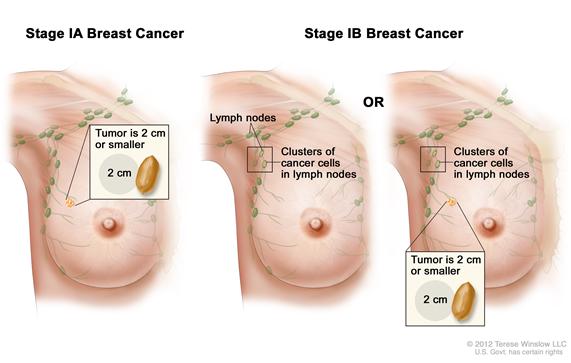
In stage I, cancer has formed. Stage I is divided into stages IA and IB.
- In stage IA, the tumor is 2 centimeters or smaller. Cancer has not spread outside the breast.
- In stage IB, small clusters of breast cancer cells (larger than 0.2 millimeter but not larger than 2 millimeters) are found in the lymph nodes and either:
- no tumor is found in the breast; or
- the tumor is 2 centimeters or smaller.
Stage II is divided into stages IIA and IIB.
- In stage IIA:
- no tumor is found in the breast or the tumor is 2 centimeters or smaller. Cancer (larger than 2 millimeters) is found in 1 to 3 axillary lymph nodes or in the lymph nodes near the breastbone (found during a sentinel lymph node biopsy); or
- the tumor is larger than 2 centimeters but not larger than 5 centimeters. Cancer has not spread to the lymph nodes.
Enlarge
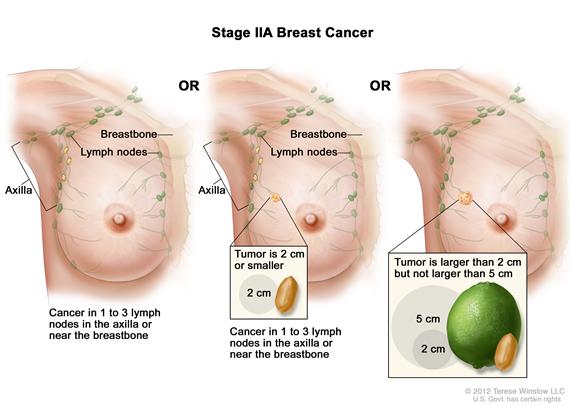 Stage IIA breast cancer. No tumor is found in the breast and cancer is found in 1 to 3 axillary lymph nodes or lymph nodes near the breastbone (left panel); OR the tumor is 2 centimeters or smaller and cancer is found in 1 to 3 axillary lymph nodes or lymph nodes near the breastbone (middle panel); OR the tumor is larger than 2 centimeters but not larger than 5 centimeters and has not spread to the lymph nodes (right panel).
Stage IIA breast cancer. No tumor is found in the breast and cancer is found in 1 to 3 axillary lymph nodes or lymph nodes near the breastbone (left panel); OR the tumor is 2 centimeters or smaller and cancer is found in 1 to 3 axillary lymph nodes or lymph nodes near the breastbone (middle panel); OR the tumor is larger than 2 centimeters but not larger than 5 centimeters and has not spread to the lymph nodes (right panel). - In stage IIB, the tumor is:
- larger than 2 centimeters but not larger than 5 centimeters. Small clusters of breast cancer cells (larger than 0.2 millimeter but not larger than 2 millimeters) are found in the lymph nodes; or
- larger than 2 centimeters but not larger than 5 centimeters. Cancer has spread to 1 to 3 axillary lymph nodes or to the lymph nodes near the breastbone (found during a sentinel lymph node biopsy); or
- larger than 5 centimeters. Cancer has not spread to the lymph nodes.
Enlarge
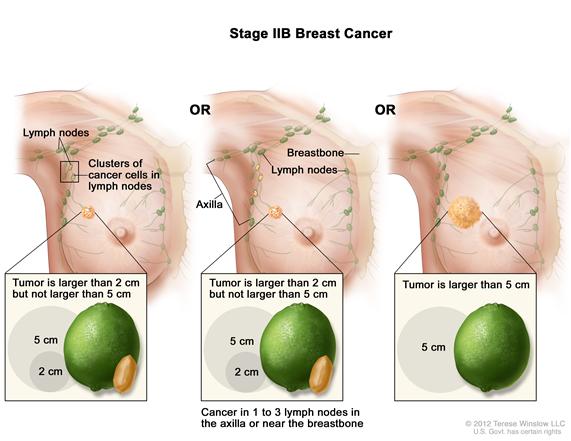 Stage IIB breast cancer. The tumor is larger than 2 centimeters but not larger than 5 centimeters and small clusters of cancer cells are found in the lymph nodes (left panel); OR the tumor is larger than 2 centimeters but not larger than 5 centimeters and cancer is found in 1 to 3 axillary lymph nodes or lymph nodes near the breastbone (middle panel); OR the tumor is larger than 5 centimeters and has not spread to the lymph nodes (right panel).
Stage IIB breast cancer. The tumor is larger than 2 centimeters but not larger than 5 centimeters and small clusters of cancer cells are found in the lymph nodes (left panel); OR the tumor is larger than 2 centimeters but not larger than 5 centimeters and cancer is found in 1 to 3 axillary lymph nodes or lymph nodes near the breastbone (middle panel); OR the tumor is larger than 5 centimeters and has not spread to the lymph nodes (right panel).
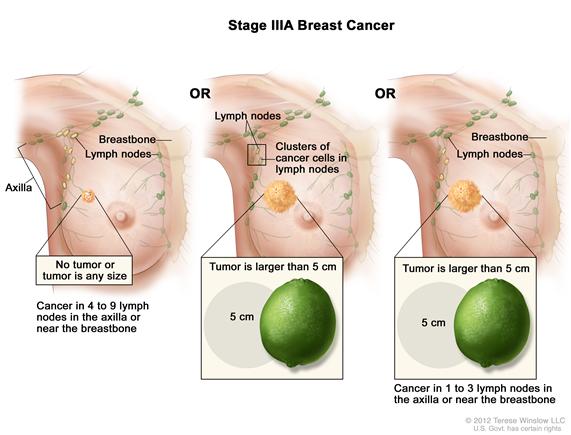
In stage IIIA:
- no tumor is found in the breast or the tumor may be any size. Cancer is found in 4 to 9 axillary lymph nodes or in the lymph nodes near the breastbone (found during imaging tests or a physical exam); or
- the tumor is larger than 5 centimeters. Small clusters of breast cancer cells (larger than 0.2 millimeter but not larger than 2 millimeters) are found in the lymph nodes; or
- the tumor is larger than 5 centimeters. Cancer has spread to 1 to 3 axillary lymph nodes or to the lymph nodes near the breastbone (found during a sentinel lymph node biopsy).
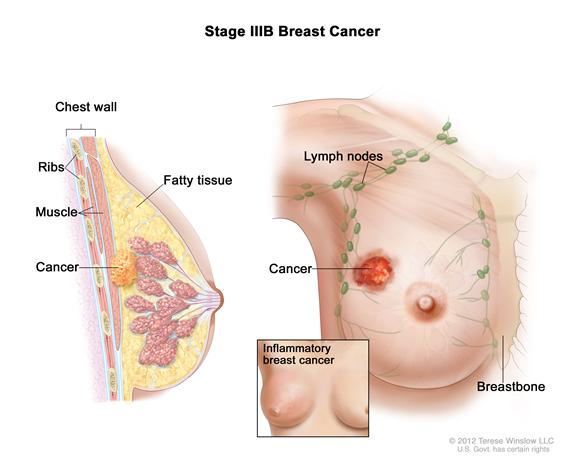
In stage IIIB, the tumor may be any size and cancer has spread to the chest wall and/or to the skin of the breast and caused swelling or an ulcer. Also, cancer may have spread to:
- up to 9 axillary lymph nodes; or
- the lymph nodes near the breastbone.
Cancer that has spread to the skin of the breast may also be inflammatory breast cancer. See the section on Inflammatory Breast Cancer for more information.
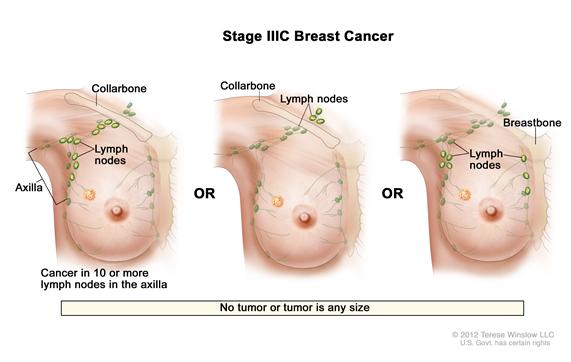
In stage IIIC, no tumor is found in the breast or the tumor may be any size. Cancer may have spread to the skin of the breast and caused swelling or an ulcer and/or has spread to the chest wall. Also, cancer has spread to:
- 10 or more axillary lymph nodes; or
- lymph nodes above or below the collarbone; or
- axillary lymph nodes and lymph nodes near the breastbone.
Cancer that has spread to the skin of the breast may also be inflammatory breast cancer. See the section on Inflammatory Breast Cancer for more information.
For treatment, stage IIIC breast cancer is divided into operable and inoperable stage IIIC.
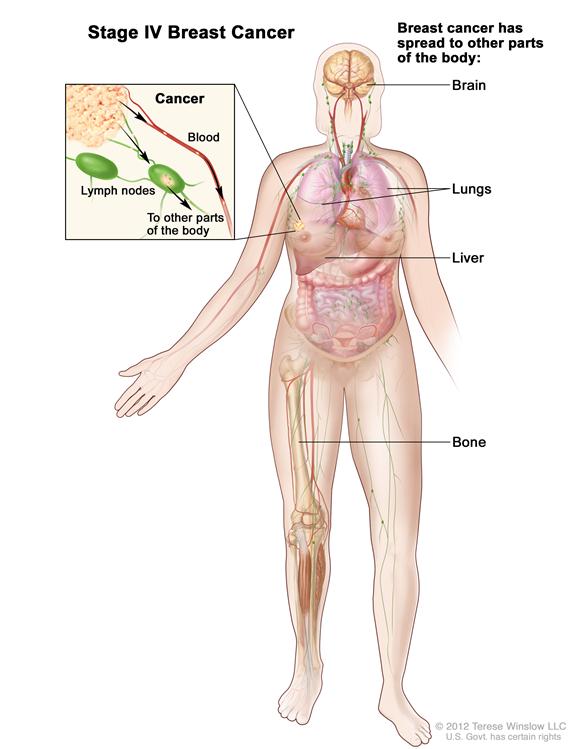
In stage IV, cancer has spread to other organs of the body, most often the bones, lungs, liver, or brain.
Inflammatory Breast Cancer
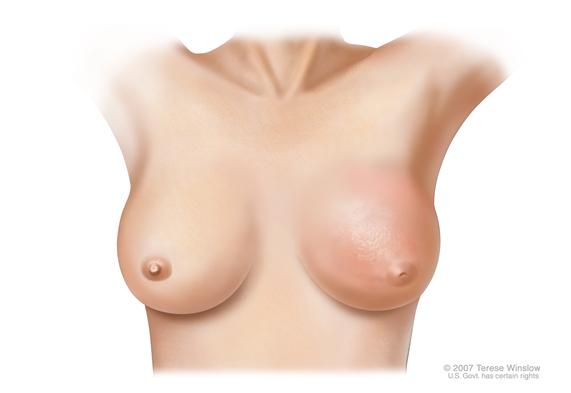
In inflammatory breast cancer, cancer has spread to the skin of the breast and the breast looks red and swollen and feels warm. The redness and warmth occur because the cancer cells block the lymph vessels in the skin. The skin of the breast may also show the dimpled appearance called peau d’orange (like the skin of an orange). There may not be any lumps in the breast that can be felt. Inflammatory breast cancer may be stage IIIB, stage IIIC, or stage IV.
Recurrent Breast Cancer
Recurrent breast cancer is cancer that has recurred (come back) after it has been treated. The cancer may come back in the breast, in the chest wall, or in other parts of the body.
Treatment Option Overview
Key Points for This Section
- There are different types of treatment for patients with breast cancer.
- Six types of standard treatment are used:
- New types of treatment are being tested in clinical trials.
- Patients may want to think about taking part in a clinical trial.
- Patients can enter clinical trials before, during, or after starting their cancer treatment.
- Follow-up tests may be needed.
There are different types of treatment for patients with breast cancer.
Different types of treatment are available for patients with breast cancer. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Six types of standard treatment are used:
Most patients with breast cancer have surgery to remove the cancer from the breast. Some of the lymph nodes under the arm are usually taken out and looked at under a microscope to see if they contain cancer cells.
Breast-conserving surgery, an operation to remove the cancer but not the breast itself, includes the following:
- Lumpectomy: Surgery to remove a tumor (lump) and a small amount of normal tissue around it.
- Partial mastectomy: Surgery to remove the part of the breast that has cancer and some normal tissue around it. The lining over the chest muscles below the cancer may also be removed. This procedure is also called a segmental mastectomy.
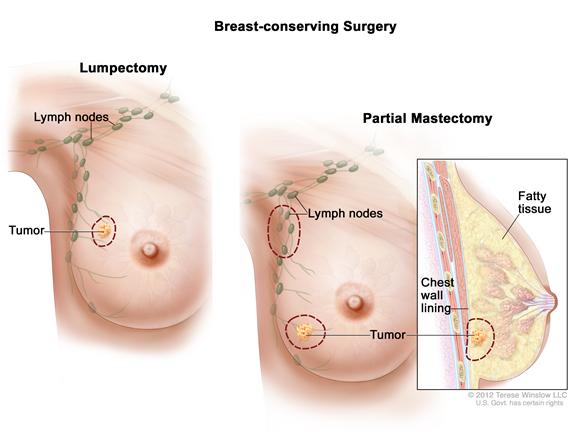
Patients who are treated with breast-conserving surgery may also have some of the lymph nodes under the arm removed for biopsy. This procedure is called lymph node dissection. It may be done at the same time as the breast-conserving surgery or after. Lymph node dissection is done through a separate incision.
Other types of surgery include the following:
- Total mastectomy: Surgery to remove the whole breast that has cancer. This procedure is also called a simple mastectomy. Some of the lymph nodes under the arm may be removed for biopsy at the same time as the breast surgery or after. This is done through a separate incision. Enlarge
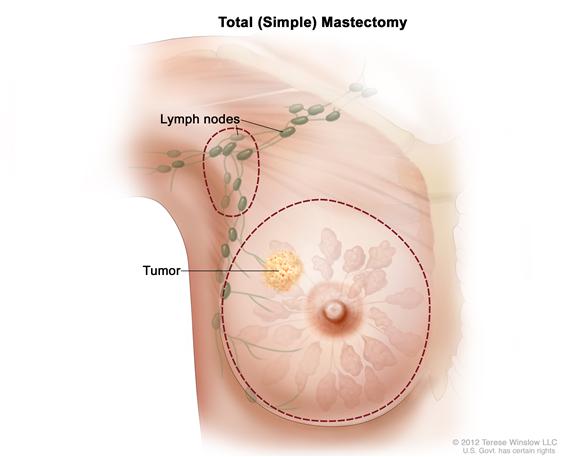 Total (simple) mastectomy. The dotted line shows where the entire breast is removed. Some lymph nodes under the arm may also be removed.
Total (simple) mastectomy. The dotted line shows where the entire breast is removed. Some lymph nodes under the arm may also be removed. - Modified radical mastectomy: Surgery to remove the whole breast that has cancer, many of the lymph nodes under the arm, the lining over the chest muscles, and sometimes, part of the chest wall muscles. Enlarge
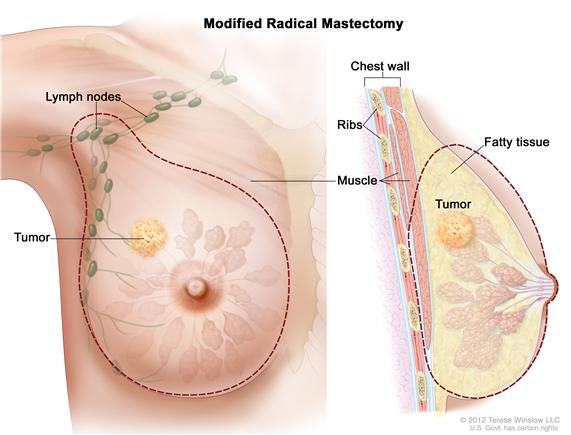 Modified radical mastectomy. The dotted line shows where the entire breast and some lymph nodes are removed. Part of the chest wall muscle may also be removed.
Modified radical mastectomy. The dotted line shows where the entire breast and some lymph nodes are removed. Part of the chest wall muscle may also be removed.
Chemotherapy may be given before surgery to remove the tumor. When given before surgery, chemotherapy will shrink the tumor and reduce the amount of tissue that needs to be removed during surgery. Treatment given before surgery is called neoadjuvant therapy.
Even if the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given radiation therapy, chemotherapy, or hormone therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
If a patient is going to have a mastectomy, breast reconstruction (surgery to rebuild a breast’s shape after a mastectomy) may be considered. Breast reconstruction may be done at the time of the mastectomy or at a future time. The reconstructed breast may be made with the patient’s own (nonbreast) tissue or by using implants filled with saline or silicone gel. Before the decision to get an implant is made, patients can call the Food and Drug Administration's (FDA) Center for Devices and Radiologic Health at 1-888-INFO-FDA (1-888-463-6332) or visit the FDA's Web site for more information on breast implants.
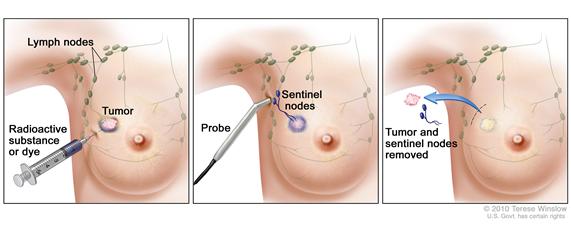
Sentinel lymph node biopsy followed by surgery
Sentinel lymph node biopsy is the removal of the sentinel lymph node during surgery. The sentinel lymph node is the first lymph node to receive lymphatic drainage from a tumor. It is the first lymph node the cancer is likely to spread to from the tumor. A radioactive substance and/or blue dye is injected near the tumor. The substance or dye flows through the lymph ducts to the lymph nodes. The first lymph node to receive the substance or dye is removed. A pathologist views the tissue under a microscope to look for cancer cells. If cancer cells are not found, it may not be necessary to remove more lymph nodes. After the sentinel lymph node biopsy, the surgeon removes the tumor (breast-conserving surgery or mastectomy).
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy. External radiation therapy uses a machine outside the body to send radiation toward the cancer. Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer. The way the radiation therapy is given depends on the type and stage of the cancer being treated.
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type and stage of the cancer being treated.
See Drugs Approved for Breast Cancer for more information.
Hormone therapy is a cancer treatment that removes hormones or blocks their action and stops cancer cells from growing. Hormones are substances made by glands in the body and circulated in the bloodstream. Some hormones can cause certain cancers to grow. If tests show that the cancer cells have places where hormones can attach (receptors), drugs, surgery, or radiation therapy is used to reduce the production of hormones or block them from working. The hormone estrogen, which makes some breast cancers grow, is made mainly by the ovaries. Treatment to stop the ovaries from making estrogen is called ovarian ablation.
Hormone therapy with tamoxifen is often given to patients with early stages of breast cancer and those with metastatic breast cancer (cancer that has spread to other parts of the body). Hormone therapy with tamoxifen or estrogens can act on cells all over the body and may increase the chance of developing endometrial cancer. Women taking tamoxifen should have a pelvic exam every year to look for any signs of cancer. Any vaginal bleeding, other than menstrual bleeding, should be reported to a doctor as soon as possible.
Hormone therapy with an aromatase inhibitor is given to some postmenopausal women who have hormone-dependent breast cancer. Hormone-dependent breast cancer needs the hormone estrogen to grow. Aromatase inhibitors decrease the body's estrogen by blocking an enzyme called aromatase from turning androgen into estrogen.
For the treatment of early stage breast cancer, certain aromatase inhibitors may be used as adjuvant therapy instead of tamoxifen or after 2 or more years of tamoxifen. For the treatment of metastatic breast cancer, aromatase inhibitors are being tested in clinical trials to compare them to hormone therapy with tamoxifen.
See Drugs Approved for Breast Cancer for more information.
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells without harming normal cells. Monoclonal antibodies and tyrosine kinase inhibitors are two types of targeted therapies used in the treatment of breast cancer. PARP inhibitors are a type of targeted therapy being studied for the treatment of triple-negative breast cancer.
Monoclonal antibody therapy is a cancer treatment that uses antibodies made in the laboratory, from a single type of immune system cell. These antibodies can identify substances on cancer cells or normal substances that may help cancer cells grow. The antibodies attach to the substances and kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells. Monoclonal antibodies may be used in combination with chemotherapy as adjuvant therapy.
Trastuzumab is a monoclonal antibody that blocks the effects of the growth factor protein HER2, which sends growth signals to breast cancer cells. About one-fourth of patients with breast cancer have tumors that may be treated with trastuzumab combined with chemotherapy.
Pertuzumab is a monoclonal antibody that may be combined with trastuzumab and chemotherapy to treat breast cancer. It may be used to treat certain patients with HER2-positive breast cancer that has metastasized (spread to other parts of the body).
Tyrosine kinase inhibitors are targeted therapy drugs that block signals needed for tumors to grow. Tyrosine kinase inhibitors may be used with other anticancer drugs as adjuvant therapy.
Lapatinib is a tyrosine kinase inhibitor that blocks the effects of the HER2 protein and other proteins inside tumor cells. It may be used with other drugs to treat patients with HER2-positive breast cancer that has progressed after treatment with trastuzumab.
PARP inhibitors are a type of targeted therapy that block DNA repair and may cause cancer cells to die. PARP inhibitor therapy is being studied for the treatment of triple-negative breast cancer.
See Drugs Approved for Breast Cancer for more information.
New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI Web site.
High-dose chemotherapy with stem cell transplant
High-dose chemotherapy with stem cell transplant is a way of giving high doses of chemotherapy and replacing blood -forming cells destroyed by the cancer treatment. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the chemotherapy is completed, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body’s blood cells.
Studies have shown that high-dose chemotherapy followed by stem cell transplant does not work better than standard chemotherapy in the treatment of breast cancer. Doctors have decided that, for now, high-dose chemotherapy should be tested only in clinical trials. Before taking part in such a trial, women should talk with their doctors about the serious side effects, including death, that may be caused by high-dose chemotherapy.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. See the Treatment Options section that follows for links to current treatment clinical trials. These have been retrieved from NCI's listing of clinical trials.
Follow-up tests may be needed.
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests. This is sometimes called re-staging.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back). These tests are sometimes called follow-up tests or check-ups.
Treatment Options by Stage
A link to a list of current clinical trials is included for each treatment section. For some types or stages of cancer, there may not be any trials listed. Check with your doctor for clinical trials that are not listed here but may be right for you.
Ductal Carcinoma In Situ (DCIS)Treatment of ductal carcinoma in situ (DCIS) may include the following:
- Breast-conserving surgery and radiation therapy with or without tamoxifen.
- Total mastectomy with or without tamoxifen.
- Breast-conserving surgery without radiation therapy.
- Clinical trials testing breast-conserving surgery and tamoxifen with or without radiation therapy.
Check for U.S. clinical trials from NCI's list of cancer clinical trials that are now accepting patients with ductal breast carcinoma in situ. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. General information about clinical trials is available from the NCI Web site.
Lobular Carcinoma In Situ (LCIS)Treatment of lobular carcinoma in situ (LCIS) may include the following:
- Biopsy to diagnose the LCIS followed by regular examinations and regular mammograms to find any changes as early as possible. This is called observation.
- Tamoxifen to reduce the risk of developing breast cancer.
- Bilateral prophylactic mastectomy. This treatment choice is sometimes used in women who have a high risk of getting breast cancer. Most surgeons believe that this is a more aggressive treatment than is needed.
- Clinical trials testing cancer prevention drugs.
Check for U.S. clinical trials from NCI's list of cancer clinical trials that are now accepting patients with lobular breast carcinoma in situ. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. General information about clinical trials is available from the NCI Web site.
Stage I, Stage II, Stage IIIA, and Operable Stage IIIC Breast CancerTreatment of stage I, stage II, stage IIIA, and operable stage IIIC breast cancer may include the following:
- Breast-conserving surgery to remove only the cancer and some surrounding breast tissue, followed by lymph node dissection and radiation therapy.
- Modified radical mastectomy with or without breast reconstruction surgery.
- Sentinel lymph node biopsy followed by surgery.
Adjuvant therapy (treatment given after surgery to lower the risk that cancer will come back) may include the following:
- Radiation therapy to the lymph nodes near the breast and to the chest wall after a modified radical mastectomy.
- Chemotherapy with or without hormone therapy.
- Hormone therapy.
- Monoclonal antibody therapy with trastuzumab combined with chemotherapy.
- A clinical trial of new targeted therapies.
Check for U.S. clinical trials from NCI's list of cancer clinical trials that are now accepting patients with stage I breast cancer, stage II breast cancer, stage IIIA breast cancer and stage IIIC breast cancer. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. General information about clinical trials is available from the NCI Web site.
Stage IIIB, Inoperable Stage IIIC, Stage IV, and Metastatic Breast CancerStage IIIB and inoperable stage IIIC breast cancer
Treatment of stage IIIB and inoperable stage IIIC breast cancer may include the following:
- Chemotherapy.
- Chemotherapy followed by surgery (breast-conserving surgery or total mastectomy), with lymph node dissection followed by radiation therapy. Additional therapy (chemotherapy, hormone therapy, or both) may be given.
- Clinical trials testing new anticancer drugs, new drug combinations, and new ways of giving treatment.
Treatment of stage IV or metastatic breast cancer may include the following:
- Hormone therapy and/or chemotherapy with or without trastuzumab.
- Monoclonal antibody therapy with trastuzumab and pertuzumab combined with chemotherapy.
- Tyrosine kinase inhibitor therapy with lapatinib combined with capecitabine.
- Radiation therapy and/or surgery for relief of pain and other symptoms.
- Bisphosphonate drugs to reduce bone disease and pain when cancer has spread to the bone.
- Clinical trials testing new chemotherapy and/or hormone therapy.
- Clinical trials of new combinations of treatments, including targeted therapy, hormone therapy, and chemotherapy.
- Clinical trials testing other approaches, including high-dose chemotherapy with stem cell transplant.
Check for U.S. clinical trials from NCI's list of cancer clinical trials that are now accepting patients with stage IIIB breast cancer, stage IIIC breast cancer and stage IV breast cancer. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. General information about clinical trials is available from the NCI Web site.
Treatment Options for Inflammatory Breast Cancer
Treatment of inflammatory breast cancer may include the following:
- Chemotherapy.
- Chemotherapy followed by surgery (breast-conserving surgery or total mastectomy), with lymph node dissection followed by radiation therapy. Additional therapy (chemotherapy, hormone therapy, or both) may be given.
- Clinical trials testing new anticancer drugs, new drug combinations, and new ways of giving treatment.
Check for U.S. clinical trials from NCI's list of cancer clinical trials that are now accepting patients with inflammatory breast cancer. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. General information about clinical trials is available from the NCI Web site.
Treatment Options for Triple-Negative Breast Cancer
Treatment of triple-negative breast cancer may include the following:
- Chemotherapy followed by surgery (breast-conserving surgery, total mastectomy, or modified radical mastectomy) and lymph node dissection.
- A clinical trial of combination chemotherapy with drugs that are often used to treat breast cancer and drugs that are not usually used to treat breast cancer.
- A clinical trial of PARP inhibitor therapy.
Check for U.S. clinical trials from NCI's list of cancer clinical trials that are now accepting patients with triple-negative breast cancer. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. General information about clinical trials is available from the NCI Web site.
Treatment Options for Recurrent Breast Cancer
Treatment of recurrent breast cancer (cancer that has come back after treatment) in the breast or chest wall may include the following:
- Surgery (modified radical mastectomy), radiation therapy, or both.
- Chemotherapy or hormone therapy.
- A clinical trial of trastuzumab combined with chemotherapy.
Check for U.S. clinical trials from NCI's list of cancer clinical trials that are now accepting patients with recurrent breast cancer. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. General information about clinical trials is available from the NCI Web site.
To Learn More About Breast Cancer
For more information from the National Cancer Institute about breast cancer, see the following:
- Breast Cancer Home Page
- What You Need to Know About™ Breast Cancer
- Breast Cancer Prevention
- Breast Cancer Screening
- Breast Cancer Treatment and Pregnancy
- Preventive Mastectomy
- Sentinel Lymph Node Biopsy
- Drugs Approved for Breast Cancer
- Hormone Therapy for Breast Cancer
- Understanding Cancer Series: Targeted Therapies (Advances in Targeted Therapies and Targeted Therapies for Breast Cancer)
- Targeted Cancer Therapies
- Inflammatory Breast Cancer: Questions and Answers
- BRCA1 and BRCA2: Cancer Risk and Genetic Testing
For general cancer information and other resources from the National Cancer Institute, see the following:
- What You Need to Know About™ Cancer
- Understanding Cancer Series: Cancer
- Cancer Staging
- Chemotherapy and You: Support for People With Cancer
- Radiation Therapy and You: Support for People With Cancer
- Coping with Cancer: Supportive and Palliative Care
- Questions to Ask Your Doctor About Cancer
- Cancer Library
- Information For Survivors/Caregivers/Advocates
Changes to This Summary (10/03/2012)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
Images were added to this summary.
Get More Information From NCI
Call 1-800-4-CANCER
For more information, U.S. residents may call the National Cancer Institute's (NCI's) Cancer Information Service toll-free at 1-800-4-CANCER (1-800-422-6237) Monday through Friday from 8:00 a.m. to 8:00 p.m., Eastern Time. A trained Cancer Information Specialist is available to answer your questions.
Chat online
The NCI's LiveHelp® online chat service provides Internet users with the ability to chat online with an Information Specialist. The service is available from 8:00 a.m. to 11:00 p.m. Eastern time, Monday through Friday. Information Specialists can help Internet users find information on NCI Web sites and answer questions about cancer.
Write to us
For more information from the NCI, please write to this address:
- NCI Public Inquiries Office
- Suite 3036A
- 6116 Executive Boulevard, MSC8322
- Bethesda, MD 20892-8322
Search the NCI Web site
The NCI Web site provides online access to information on cancer, clinical trials, and other Web sites and organizations that offer support and resources for cancer patients and their families. For a quick search, use the search box in the upper right corner of each Web page. The results for a wide range of search terms will include a list of "Best Bets," editorially chosen Web pages that are most closely related to the search term entered.
There are also many other places to get materials and information about cancer treatment and services. Hospitals in your area may have information about local and regional agencies that have information on finances, getting to and from treatment, receiving care at home, and dealing with problems related to cancer treatment.
Find Publications
The NCI has booklets and other materials for patients, health professionals, and the public. These publications discuss types of cancer, methods of cancer treatment, coping with cancer, and clinical trials. Some publications provide information on tests for cancer, cancer causes and prevention, cancer statistics, and NCI research activities. NCI materials on these and other topics may be ordered online or printed directly from the NCI Publications Locator. These materials can also be ordered by telephone from the Cancer Information Service toll-free at 1-800-4-CANCER (1-800-422-6237).
About PDQ
PDQ is a comprehensive cancer database available on NCI's Web site.
PDQ is the National Cancer Institute's (NCI's) comprehensive cancer information database. Most of the information contained in PDQ is available online at NCI's Web site. PDQ is provided as a service of the NCI. The NCI is part of the National Institutes of Health, the federal government's focal point for biomedical research.
PDQ contains cancer information summaries.
The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries are available in two versions. The health professional versions provide detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions provide current and accurate cancer information.
Images in the PDQ summaries are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in the PDQ summaries, along with many other cancer-related images, are available in Visuals Online, a collection of over 2,000 scientific images.
The PDQ cancer information summaries are developed by cancer experts and reviewed regularly.
Editorial Boards made up of experts in oncology and related specialties are responsible for writing and maintaining the cancer information summaries. The summaries are reviewed regularly and changes are made as new information becomes available. The date on each summary ("Date Last Modified") indicates the time of the most recent change.
PDQ also contains information on clinical trials.
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become "standard." Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Listings of clinical trials are included in PDQ and are available online at NCI's Web site. Descriptions of the trials are available in health professional and patient versions. Many cancer doctors who take part in clinical trials are also listed in PDQ. For more information, call the Cancer Information Service 1-800-4-CANCER (1-800-422-6237).