
You are here: Home > Triage Guidelines
Triage Guidelines

- Triage of Chemical Casualties
- Key Activities for Triage
- START/JumpSTART Algorithm (Simple Triage and Rapid Treatment) for Mass Casualty Events
- SALT Mass Casualty Triage Algorithm
Triage of Chemical Casualties
General principles of triage for chemical exposures
- Check triage tag/card for any previous treatment or triage.
- Survey for evidence of associated traumatic/blast injuries.
- Observe for sweating, labored breathing, coughing/vomiting, secretions.
- Severe casualty triaged as immediate if assisted breathing is required.
- Blast injuries or other trauma, where there is question whether there is chemical exposure, victims must be tagged as immediate in most cases. Blast victim's evidence delayed effects such as ARDS, etc.
- Mild/moderate casualty: self/buddy aid, triaged as delayed or minimal and release is based on strict follow up and instructions.
- If there are chemical exposure situations which may cause delayed but serious signs and symptoms, then over-triage is considered appropriate to the proper facilities that can observe and manage any delayed onset symptoms.
- Expectant categories in multi-casualty events are those victims who have experienced a cardiac arrest, respiratory arrest, or continued seizures immediately. Resources should not be expended on these casualties if there are large numbers of casualties requiring care and transport with minimal or scant resources available.
- In a given category prioritize a child, pregnant woman over an non-pregnant adult
Chemical agent-specific triage
See Triage Sections of Prehospital and Hospital Management:
Key Activities for Triage 1
- The dose determines the poison during triage. Determining if a patient had direct contact (e.g., splash or skin contact) and the relative distance from areas with the highest concentrations (e.g., near the source of a leak or spill) can guide triage decisions, just like principles of radiation dose delivery (i.e, time, shielding, distance) apply to many mass chemical events.
- Obtaining history about the time a patient was in a toxic environment and the distance from the areas of greatest concentration can help to stratify patients into high-risk and low-risk groups. This approach is similar to using an account of the mechanism of injury to anticipate injuries even before the clinician touches the trauma patient.
- Understanding the different mechanisms of trauma (e.g., speed of the vehicle, presence of fatalities in the same accident, or height of a fall) and the predictable pattern of injuries that may result will influence the patient's evaluation and affect care. This approach is not an absolute solution for poisonings but is potentially valuable for mass chemical exposures whereby triaging patients is critical to quickly find those most at risk for serious illness.
- In addition to triage, the same principles can guide treatment strategies for hazardous chemical exposures.
- The most basic treatment objective is to limit exposure time and decrease concentration as rapidly as possible. Moving rapidly away from a vapor cloud in an accidental release is common sense and illustrates the point of decreasing concentration and duration of exposure. Similarly, deluging with water after splashing a concentrated sulfuric acid on the skin will decrease the chemical's concentration and the duration of exposure.
START/JumpSTART Algorithm (Simple Triage and Rapid Treatment) for Mass Casualty Events
START was developed by the Newport Beach Fire and Marine Department and Hoag Hospital in Newport Beach, California in 1983.
Initially it used the ability to obey commands, respiratory rate, and capillary refill to assign triage category.
Modifications to START in 1996 by Benson et. al. substituted radial pulse for capillary refill, with a report of improved accuracy, especially in cold temperature.

JumpSTART, a pediatric version of START, was developed at the Miami, Florida Children's Hospital in 1995 by Dr. Lou Romig.
A modification was published in 2001. Formal scientific review of the efficacy of JumpStart has been limited.
JumpSTART is probably the most commonly used pediatric mass casualty triage algorithm in the US.
SALT Mass Casualty Triage Algorithm
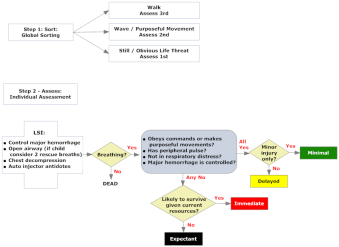
SALT stands for "Sort - Assess - Life Saving Interventions - Treatment and/or Transport"
It was developed as a national all-hazards mass casualty initial triage standard for all patients.
Agencies can easily incorporate SALT into their current Mass Casualty Incident (MCI) triage protocol through simple modification.
References
- Kirk MA, Deaton ML. Bringing order out of chaos: effective strategies for medical response to mass chemical exposure. Emerg Med Clin North Am. 2007 May;25(2):527-48. [PubMed Citation]
- Triage of Chemical Casualties, Medical Aspects of Chemical Warfare, Chapter 15 (PDF - 285 KB) (U.S. Army, 2008)
- Subbarao I, Johnson C, Bond WF, Schwid HA, Wasser TE, Deye GA, Burkhart KK. Symptom-based, algorithmic approach for handling the initial encounter with victims of a potential terrorist attack. Prehosp Disaster Med. 2005 Sep-Oct;20(5):301-8. [PubMed Citation]
- Cone DC, Koenig KL. Mass casualty triage in the chemical, biological, radiological, or nuclear environment. Eur J Emerg Med. 2005 Dec;12(6):287-302. [PubMed Citation]
- Cone DC, MacMillan DS, Parwani V, Van Gelder C. Pilot test of a proposed chemical/biological/radiation/ nuclear-capable mass casualty triage system. Prehosp Emerg Care. 2008 Apr-Jun;12(2):236-40. [PubMed Citation]
PDF documents can be viewed with the free Adobe® Reader™
