NIDDK FY2011 President’s Budget Request
NATIONAL INSTITUTES OF HEALTH
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)
FY 2011 Budget
Print Version (PDF 749KB, 30 pages) 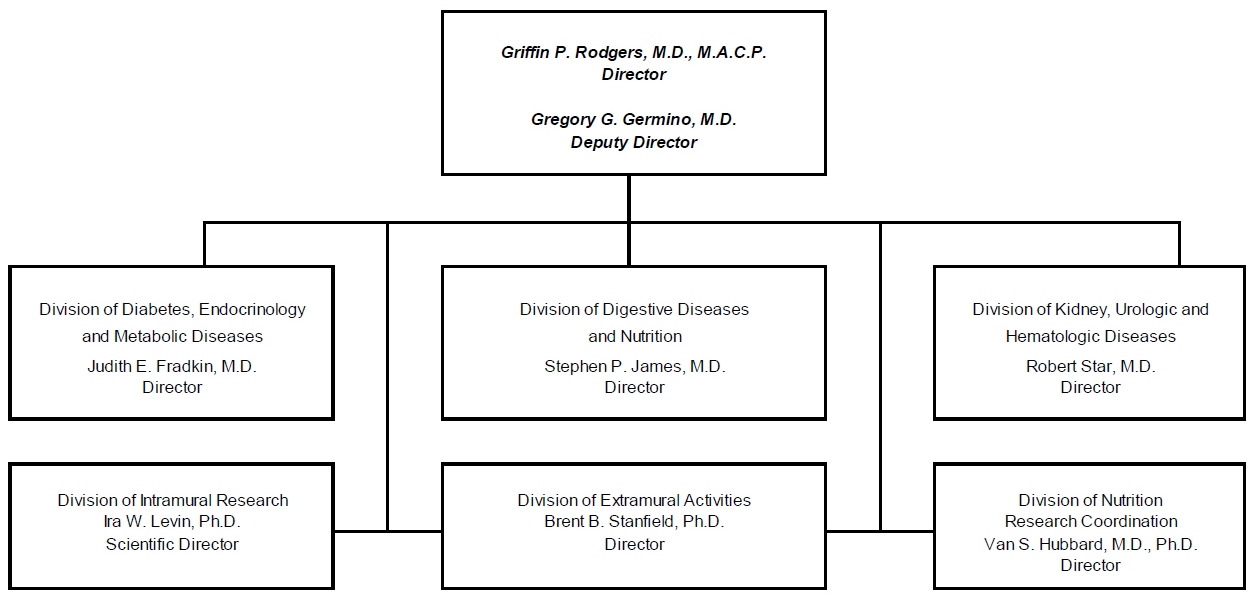
For carrying out section 301 and title IV of the Public Health Services Act with respect to diabetes and digestive and kidney diseases [$1,808,100,000] $1,857,589,000 (Public Law 111-117, Consolidated Appropriations Act, 2010)
Amounts Available for Obligation 1/| Source of Funding | FY 2009
Actual | FY 2010
Estimate | FY 2011
PB |
|---|
| Appropriation | $1,761,338,000 | $1,808,100,000 | $1,857,589,000 |
| Type 1 Diabetes 2/ | 150,000,000 | 150,000,000 | 150,000,000 |
| Subtotal, adjusted appropriation | 1,911,338,000 | 1,958,100,000 | 2,007,589,000 |
| Real transfer under Director's one-percent transfer authority (GEI) | 1,165,000 | 0 | 0 |
| Real transfer to the Office of AIDS Research | -625,000 | 0 | 0 |
| Comparative transfer to the National Library of Medicine for the National Center for Biotechnology Information and Public Access | -562,000 | -736,000 | 0 |
| Comparative transfer under Director's one-percent transfer authority (GEI) | -1,165,000 | 0 | 0 |
| Subtotal, adjusted budget authority | 1,910,151,000 | 1,957,364,000 | 2,007,589,000 |
| Unobligated balance lapsing | -83,000 | 0 | 0 |
| Total obligations | 1,910,068,000 | 1,957,364,000 | 2,007,589,000 |
1 / Excludes the following amounts for reimbursable activities carried out by this account: FY 2009 - $4,270,000 FY 2010 - $10,000,000 FY 2011 - $10,000,000 Excludes $8,853,000 Actual in FY 2009; $5,000,000 Estimate in FY 2010 and $5,000,000 Estimate in FY 2011 for royalties.
2 / Type 1 Diabetes Special Statutory Authority in Accordance with P.L. 107-360 and P.L. 110-275.
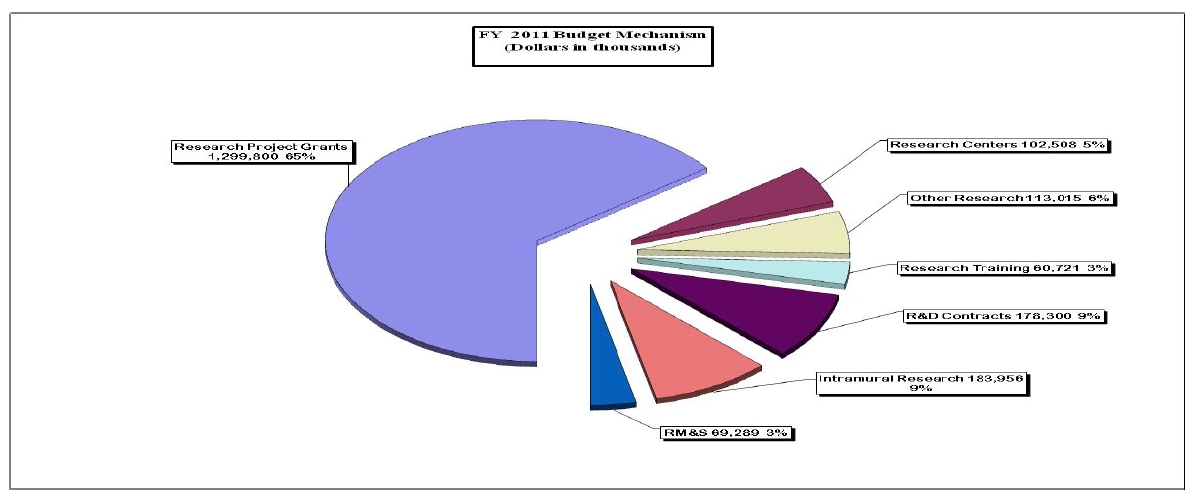
Budget Mechanism - Total
(Dollars in thousands)MECHANISM
Research Grants: | FY 2009ActualNo. | FY 2009ActualAmount | FY 2009 RecoveryAct Actual No. | FY 2009 RecoveryAct Actual Amount | FY 2010 RecoveryAct Estimated No. | FY 2010 RecoveryAct Estimated Amount | FY 2010 Estimate No. | FY 2010 Estimate Amount | FY 2011 PB No. | FY 2011 PB Amount | Change No. | Change Amount |
|---|
| Research Projects: | | | | | | | | | | | | |
| Noncompeting | 2,110 | $829,592 |
|
| 232 | $86,828 | 2,083 | $866,384 | 2,142 | $942,597 | 59 | $76,213 |
| Administrative supplements | (192) | 21,882 | (480) | 55,296 | (1,635) | 112,862 | (192) | 21,882 | (193) | 19,382 | 1 | (2,500) |
| Competing: | | |
|
| | |
| | | | | |
| Renewal | 265 | 154,592 | 42 | 14,073 | 20 | 3,533 | 278 | 159,199 | 242 | 136,212 | (36) | -22,987 |
| New | 387 | 173,962 | 220 | 84,256 | | | 404 | 178,745 | 351 | 152,935 | (53) | -25,810 |
| Supplements | 2 | 558 | 32 | 16,715 | 30 | 14,131 | 2 | 574 | 2 | 491 | 0 | -83 |
| Subtotal, competing | 654 | 329,112 | 294 | 115,044 | 50 | 17,664 | 684 | 338,518 | 595 | 289,638 | (89) | (48,880) |
| Subtotal, RPGs | 2,764 | 1,180,586 | 294 | 170,340 | 282 | 217,354 | 2,767 | 1,226,784 | 2,737 | 1,251,617 | (30) | 24,833 |
| SBIR/STTR | 119 | 46,625 | 1 | 755 | 1 | 1,015 | 122 | 47,245 | 124 | 48,183 | 2 | 938 |
| Subtotal, RPGs | 2,883 | 1,227,211 | 295 | 171,095 | 283 | 218,369 | 2,889 | 1,274,029 | 2,861 | 1,299,800 | (28) | 25,771 |
| Research Centers: | | |
|
| | |
| | | | | |
| Specialized/comprehensive | 80 | 98,496 | 1 | 16,852 | 1 | 11,186 | 80 | 99,459 | 82 | 102,459 | 2 | 3,000 |
| Clinical research | 0 | 0 |
|
| | | 0 | 0 | 0 | 0 | 0 | 0 |
| Biotechnology | 0 | 0 |
|
| | | 0 | 0 | 0 | 0 | 0 | 0 |
| Comparative medicine | 0 | 49 |
|
| | | 0 | 49 | 0 | 49 | 0 | 0 |
| Research Centers in Minority Institutions | 0 | 0 |
|
| | | 0 | 0 | 0 | 0 | 0 | 0 |
| Subtotal, Centers | 80 | 98,545 | 1 | 16,852 | 1 | 11,186 | 80 | 99,508 | 82 | 102,508 | 2 | 3,000 |
| Other Research: | | |
|
| | |
| | | | | |
| Research careers | 512 | 72,354 |
| 3,216 | | 6,160 | 506 | 71,849 | 506 | 73,849 | 0 | 2,000 |
| Cancer education | 0 | 0 |
|
| | | 0 | 0 | 0 | 0 | 0 | 0 |
| Cooperative clinical research | 0 | 3,000 |
|
| | | 0 | 3,778 | 0 | 3,891 | 0 | 113 |
| Biomedical research support | 0 | 0 |
|
| | | 0 | 0 | 0 | 0 | 0 | 0 |
| Minority biomedical research support | 0 | 54 |
|
| | | 0 | 54 | 0 | 56 | 0 | 2 |
| Other | 92 | 34,183 |
| 4,511 | 1 | 6,899 | 92 | 34,183 | 95 | 35,219 | 3 | 1,036 |
| Subtotal, Other Research | 604 | 109,591 | 0 | 7,727 | 1 | 13,059 | 598 | 109,864 | 601 | 113,015 | 3 | 3,151 |
| Total Research Grants | 3,567 | 1,435,347 | 296 | 195,674 | 285 | 242,614 | 3,567 | 1,483,401 | 3,544 | 1,515,323 | (23) | 31,922 |
| | | |
|
| | |
| | | | | |
| Research Training: | FTTPs | | FTTPs |
| FTTPs | | FTTPs | | FTTPs | | | |
| Individual awards | 215 | 9,581 | |
| | | 215 | 9,581 | 215 | 10,156 | 0 | 575 |
| Institutional awards | 927 | 47,336 | | | | | 927 | 47,821 | 927 | 50,565 | 0 | 2,744 |
| Total, Training | 1,142 | 56,917 | |
| | | 1,142 | 57,402 | 1,142 | 60,721 | 0 | 3,319 |
| | | | |
| | |
| | | | | |
| Research & development contracts | 168 | 177,415 | |
| 2 | 1,000 | 163 | 172,320 | 167 | 178,300 | 4 | 5,980 |
| (SBIR/STTR) | (2) | (78) | |
| | | (6) | (507) | (6) | (507) | (0) | (0) |
| | | | |
| | |
| | | | | |
| | FTEs | | FTEs |
| FTEs | | FTEs | | FTEs | | FTEs | |
| Intramural research | 379 | 175,618 |
| 164 | | 2,063 | 381 | 178,252 | 394 | 183,956 | 13 | 5,704 |
| Research management and support | 247 | 64,854 | 1 | 484 | 2 | 3,394 | 249 | 65,989 | 264 | 69,289 | 15 | 3,300 |
| Construction | | 0 |
|
| | |
| 0 | | 0 | | 0 |
| Buildings and Facilities | | 0 |
|
| | |
| 0 | | 0 | | 0 |
| Total, NIDDK | 626 | 1,910,151 | 296 | 196,322 | 287 | 249,071 | 630 | 1,957,364 | 658 | 2,007,589 | 28 | 50,225 |
Budget Mechanism Type 1 Diabetes Only
(Dollars in thousands)| MECHANISM | FY 2009 Actual No | FY 2009 Actual Amount | FY 2010 Estimate No. | FY 2010 Estimate Amount | FY 2011 PB No. | FY 2011 PB Amount | Change No. | Change Amount |
|---|
| Research Grants: | | | | | | | | |
| Research Projects: | | | | | | | | |
| Noncompeting | 30 | $24,183 | 47 | $38,827 | 58 | $59,549 | 11 | $20,722 |
| Administrative supplements | (1) | 5,000 | (1) | 5,000 | (2) | 2,500 | 1 | (2,500) |
| Competing: | | | | | | | | |
| Renewal | 7 | 7,916 | 5 | 5,136 | 2 | 1,683 | (3) | -3,453 |
| New | 28 | 38,829 | 18 | 25,194 | 5 | 8,258 | (13) | -16,936 |
| Supplements | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Subtotal, competing | 35 | 46,745 | 23 | 30,330 | 7 | 9,941 | (16) | (20,389) |
| Subtotal, RPGs | 65 | 75,928 | 70 | 74,157 | 65 | 71,990 | (5) | -2,167 |
| SBIR/STTR | 10 | 4,167 | 10 | 4,167 | 10 | 4,167 | 0 | 0 |
| Subtotal, RPGs | 75 | 80,095 | 80 | 78,324 | 75 | 76,157 | (5) | -2,167 |
| Research Centers: | | | | | | | | |
| Specialized/comprehensive | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Clinical research | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Biotechnology | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Comparative medicine | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Research Centers in Minority Institutions | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Subtotal, Centers | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Other Research: |
|
| | | | | | |
| Research careers | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Cancer education | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Cooperative clinical research | 0 | 3,000 | 0 | 3,778 | 0 | 3,891 | 0 | 113 |
| Biomedical research support | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Minority biomedical research support | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Other | 0 | 874 | 0 | 874 | 0 | 900 | 0 | 26 |
| Subtotal, Other Research | 0 | 3,874 | 0 | 4,652 | 0 | 4,791 | 0 | 139 |
| Total Research Grants | 75 | 83,969 | 80 | 82,976 | 75 | 80,948 | (5) | -2,028 |
| Research Training: | FTTPs | FTTPs | FTTPs | FTTPs | FTTPs | FTTPs | FTTPs | FTTPs |
|---|
| Individual awards | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Institutional awards | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total, Training | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Research & development contracts | 0 | 65,167 | 0 | 66,145 | 24 | 68,129 | 24 | 1,984 |
| (SBIR/STTR) | (0) | (0) | (0) | (0) | (0) | (0) | (0) | (0) |
| | FTEs | FTEs | FTEs | FTEs | FTEs | FTEs | FTEs | FTEs |
|---|
| Intramural research | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Research management and support | 0 | 864 | 0 | 879 | 0 | 923 | 0 | 44 |
| Construction | | 0 | | 0 | | 0 | | 0 |
| Buildings and Facilities | | 0 | | 0 | | 0 | | 0 |
| Total, NIDDK | 0 | 150,000 | 0 | 150,000 | 0 | 150,000 | 0 | 0 |
Budget Authority by Program
(Dollars in thousands)| Extramural Research | FY 2007 Actual FTEs | FY 2007 Actual Amount | FY 2008 Actual FTEs | FY 2008 Actual Amount | FY 2009 Actual FTEs | FY 2009 Actual Amount | FY 2009 Comparable FTEs | FY 2009 Comparable Amount | FY 2010 Estimate FTEs | FY 2010 Estimate Amount | FY 2011 PB FTEs | FY 2011 PB Amount | Change FTEs | Change Amount |
|---|
| Detail: | | | | | | | | | | | | | | |
| Diabetes, Endocrinology, and Metabolic Diseases | | $630,171 | | $613,897 | | $616,595 | | $615,904 | | $625,601 | | $642,113 | | 16,512 |
| Digestive Diseases and Nutrition | | 430,187 | | 442,143 | | 471,671 | | 471,136 | | 484,841 | | 497,633 | | 12,792 |
| Kidney, Urologic, and Hematologic Diseases | | 420,746 | | 426,916 | | 433,888 | | 433,503 | | 453,560 | | 465,521 | | 11,961 |
| Type 1 Diabetes | | 150,000 | | 150,000 | | 150,000 | | 150,000 | | 150,000 | | 150,000 | | |
| Subtotal, Extramural | | 1,631,104 | | 1,632,956 | | 1,672,154 | | 1,670,543 | | 1,714,002 | | 1,755,267 | | 41,265 |
| Intramural research | 414 | 164,008 | 401 | 167,851 | 379 | 175,618 | 379 | 175,618 | 381 | 178,252 | 394 | 183,956 | 13 | 5,704 |
| Res. management & support | 222 | 57,884 | 245 | 61,381 | 247 | 64,106 | 247 | 63,990 | 249 | 65,110 | 264 | 68,366 | 15 | 3,256 |
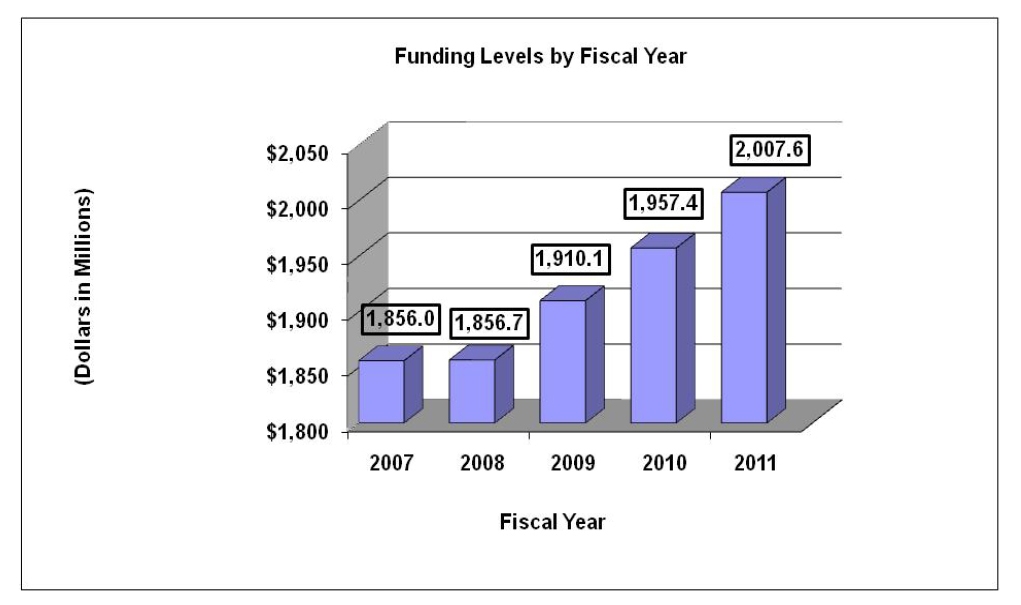
| TOTAL | 636 | 1,852,996 | 646 | 1,862,188 | 626 | 1,911,878 | 626 | 1,910,151 | 630 | 1,957,364 | 658 | 2,007,589 | 28 | 50,225 |
Major Changes in the Fiscal Year 2011 Budget Request
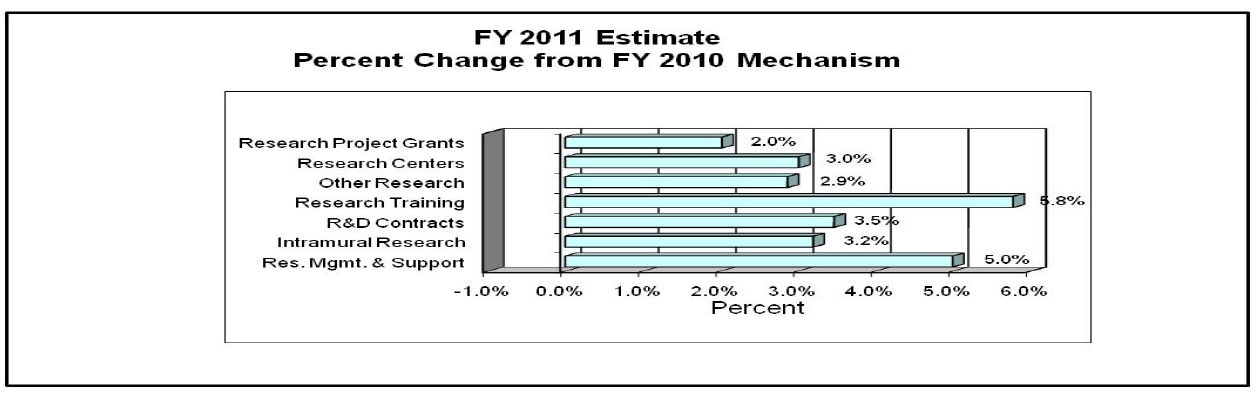
Major changes by budget mechanism and/or budget activity detail are briefly described below. Note that there may be overlap between budget mechanism and activity detail and these highlights will not sum to the total change for the FY 2011 budget request for NIDDK, which is $50.225 million more than the FY 2010 Estimate, for a total of $2,007.589 million.
Research Project Grants (RPGs; $25.771 million; total $1,299.800 million): NIDDK will award about 2,142 noncompeting RPGs for an increase of $73.713 million over FY 2010 enacted level, totaling $961.979 million in FY 2011. NIDDK will continue to maintain a 2% average cost increase of competing RPGs—595 awards in FY 2011, a decrease of 89 from FY 2010.
The Frequent Hemodialysis Network (-$1.289 million; total $.600 million): data collection will be completed during FY 2010; follow-up data analysis in FY 2011 will be less expensive.
The NIDDK acute liver failure study group ( $1.000 million; total $2.000 million): This initiative will increase by $1.000 million per year to carry out new liver failure protocols.
The NIDDK Pediatric Acute Liver Failure Study ( $2.300 million; total $3.400 million): This initiative will expand to carry out new intensive care studies of liver failure in children.
Organ Smooth Muscle: Development, Physiology, and Pathology (R01) ( $2.0 million; total $2.0 million): FY 2011 funds will support initiation of new studies of smooth muscle, which is important in hollow organ function and disease.
NIDDK Bioinformatics Grid ( $2.000 million; total $2.000 million): This effort is designed to connect several NIDDK basic science consortia (Nuclear Receptor Signaling Atlas; Beta Cell Biology Consortium; Mouse Metabolic Phenotyping Centers; Animal Models of Diabetic Complications Consortium) in a way that allows for seamless integration of the data and rapid/reciprocal exchange of this data.
Follow-up to Hyperglycemia Adverse Pregnancy Outcomes ( $4.000 million; total $4.000 million): The Hyperglycemia Adverse Pregnancy Outcomes (HAPO) Study associated glucose levels during pregnancy with perinatal outcomes. This new initiative would be to follow the children born to mothers who participated in HAPO to determine the effects of metabolic parameters during pregnancy on their subsequent growth and development.
Summary of Changes
FY 2010 Estimate: $1,957,364,000
FY 2011 estimated budget authority: 2,007,589,000
Net Change: 50,225,000
| Changes | 2010 Current Estimate
Base FTEs | 2010 Current Estimate
Base Budget Authority | Change from
Base FTEs | Change from Base
Budget Authority |
|---|
| A. Built-in: | | | | |
| 1. Intramural research: | | | | |
| a. Annualization of January | | | | |
| 2010 pay increase | | $71,748,000 | | $434,000 |
| b. January FY 2011 pay increase | | 71,748,000 | | 753,000 |
| c. Zero less days of pay (n/a for 2011) | | 71,748,000 | | 0 |
| d. Payment for centrally furnished services | | 28,513,000 | | 912,000 |
| e. Increased cost of laboratory supplies, | | | | |
| materials, and other expenses | | 77,991,000 | | 1,485,000 |
| Subtotal | | | | 3,584,000 |
| 2. Research management and support: | | | | |
| a. Annualization of January | | | | |
| 2010 pay increase | | $32,556,000 | | $197,000 |
| b. January FY 2011 pay increase | | 32,556,000 | | 342,000 |
| c. Zero less days of pay (n/a for 2011) | | 32,556,000 | | 0 |
| d. Payment for centrally furnished services | | 5,269,000 | | 169,000 |
| e. Increased cost of laboratory supplies, | | | | |
| materials, and other expenses | | 28,164,000 | | 512,000 |
| Subtotal | | | | 1,220,000 |
| Subtotal, Built-in | | | | 4,804,000 |
Summary of Changes... continued| Changes | 2010 Current Estimate
Base No. | 2010 Current Estimate
Base Budget Amount | Change from
Base No. | Change from
Base Amount |
|---|
| B. Program: | | | | |
| 1. Research project grants: | | | | |
| a. Noncompeting | 2,083 | $888,266,000 | 59 | $73,713,000 |
| b. Competing | 684 | 338,518,000 | (89) | (48,880,000) |
| c. SBIR/STTR | 122 | 47,245,000 | 2 | 938,000 |
| Total | 2,889 | 1,274,029,000 | (28) | 25,771,000 |
| 2. Research centers | 80 | 99,508,000 | 2 | 3,000,000 |
| 3. Other research | 598 | 109,864,000 | 3 | 3,151,000 |
| 4. Research training | 1,142 | 57,402,000 | 0 | 3,319,000 |
| 5. Research and development contracts | 163 | 172,320,000 | 4 | 5,980,000 |
| Subtotal, extramural | | | | 41,221,000 |
| | FTEs | FTEs | FTEs | FTEs |
| 6. Intramural research | 381 | 178,252,000 | 13 | 2,120,000 |
| 7. Research management and support | 249 | 65,989,000 | 15 | 2,080,000 |
| Subtotal, program | | 1,957,364,000 | | 45,421,000 |
| Total changes | 630 | | 28 | 50,225,000 |
Includes Type 1 Diabetes Special Statutory Authority
Justification of Budget Request
National Institute of Diabetes and Digestive and Kidney Diseases
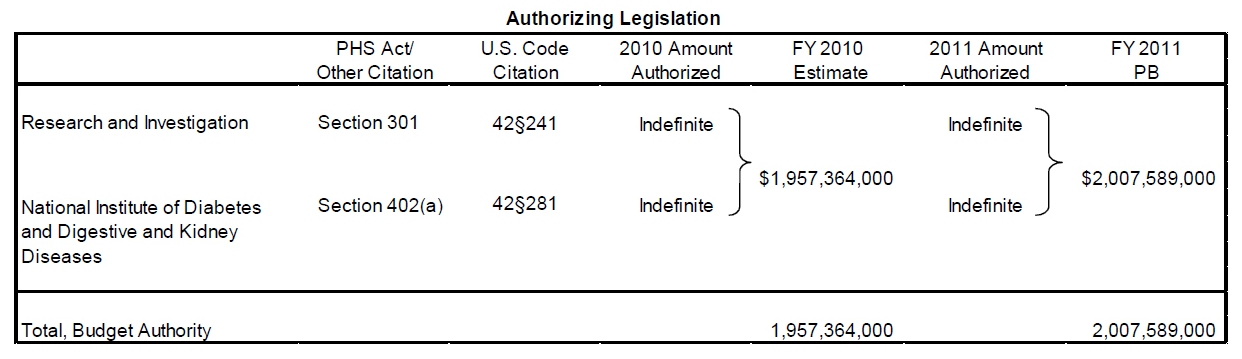
Authorizing Legislation: Section 301 and title IV of the Public Health Service Act, as amended.
Budget Authority| | FY 2009
Actual | FY 2010
Estimate | FY 2011
President’s Budget | FY 2011 /-
FY 2010 Estimate |
|---|
| BA | $1,911,338,000 | $1,958,100,000 | $2,007,589,000 | $50,552,000 |
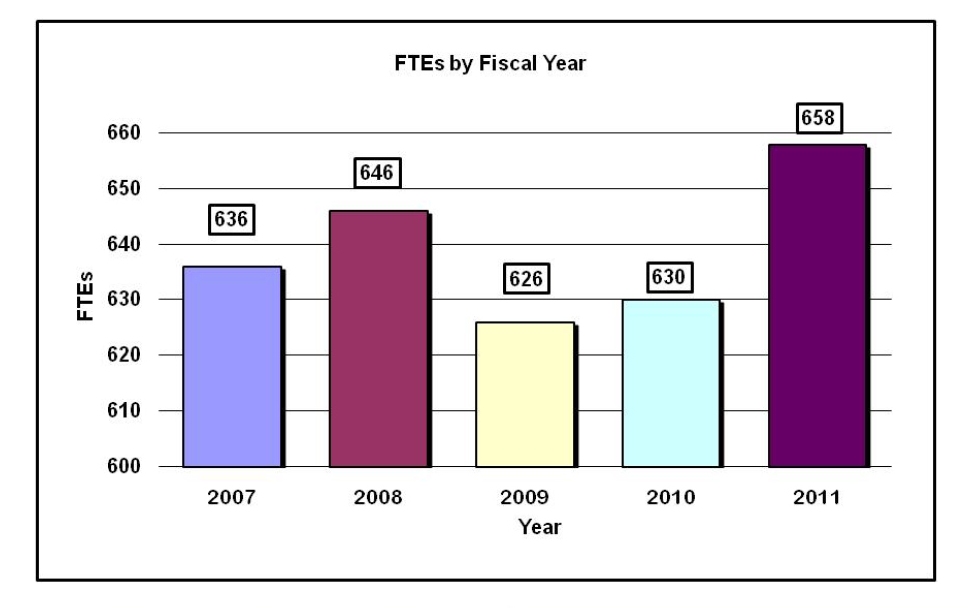
| FTEs | 626 | 630 | 658 | 28 |
| Type 1 Diabetes: | -$150,000,000 | -$150,000,000 | -$150,000,000 | |
| Labor/HHS: | $1,761,338,000 | $1,808,100,000 | $1,857,589,000 | |
This document provides justification for the Fiscal Year (FY) 2011 activities of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), including HIV/AIDS activities. Details of the FY 2011 HIV/AIDS activities are in the “Office of AIDS Research (OAR)” Section of the Overview. Details on the Common Fund are located in the Overview, Volume One. Program funds are allocated as follows: Competitive Grants/Cooperative Agreements; Contracts; Direct Federal/Intramural and Other.
DIRECTOR’S OVERVIEW
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) mission is to support and conduct research to combat diabetes and other endocrine and metabolic diseases, liver and other digestive diseases, nutritional disorders, obesity, and kidney, urologic and hematologic diseases. These diseases are chronic, common, and costly for patients, their families, and our Nation. Diabetes afflicts an estimated 23.6 million people in the U.S. and greatly increases the risk for many serious complications, such as heart disease and kidney failure.[1] An estimated 16 million U.S. adults have moderately or severely reduced kidney function; and approximately 506,000 have irreversible kidney failure.[2] Many digestive and urologic diseases are also highly prevalent.2,[3] Obesity affects approximately one-third of U.S. adults and about 16 percent of children and adolescents.[4] Obesity is a strong risk factor for type 2 diabetes, fatty liver disease, and many other diseases. Cystic fibrosis and other genetic diseases within NIDDK’s purview are less widespread, but nonetheless devastating in their impacts. Building on emerging opportunities stemming from past research investments, NIDDK will continue to pursue basic, clinical, and translational research studies; research training and career development; and health information dissemination, with a key 2010 decision to preserve its investigator-initiated research portfolio balance.
Genomics: Recent advances have greatly increased knowledge of genes associated with diabetes, kidney disease, and inflammatory bowel disease. Genomics have helped identify genetic variation affecting the likelihood of several diseases in the NIDDK mission, including inflammatory bowel disease, type 1 diabetes, type 2 diabetes, and kidney disease. NIDDK is capitalizing on these genetic findings to accelerate the development of new therapeutic approaches to these serious diseases.
Obesity: Epidemic obesity is contributing to higher rates of type 2 diabetes, the leading cause of kidney failure. To address the complex factors that promote excess weight gain, NIDDK co-chairs the NIH Obesity Research Task Force, and continues to support a multidimensional research portfolio on obesity. For example, studies are elucidating the biologic pathways that regulate appetite and energy expenditure, with implications for future therapeutic strategies. NIDDK-supported research on chronic, obesity-related conditions also includes studies of treatment for the “silent” but serious liver disease, nonalcoholic Steatohepatitis in children and adults.
Translational Research: The NIDDK is working to translate findings from basic research into new and better treatments. For example, basic research has shown that the chronic inflammation associated with obesity contributes to type 2 diabetes, heart disease, and the metabolic syndrome, suggesting that anti-inflammatory medications may be therapeutically valuable for these conditions. The Targeting Inflammation Using Salsalate for Type 2 Diabetes (TINSAL-T2D) clinical trial is testing whether the generic anti-inflammatory drug salsalate improves blood glucose control in people with type 2 diabetes. NIDDK research impacts health care reform efforts by identifying cost-effective ways to translate findings from diabetes and obesity intervention studies to real-world clinical practice and community settings. An ongoing intervention study that builds on past research is Action for Health in Diabetes (Look AHEAD,) which is testing a lifestyle intervention to help prevent common, costly, and often deadly cardiovascular complications in people with type 2 diabetes. Other NIDDK research with implications for health care reform includes comparative effectiveness research to identify the most safe and effective procedures for treating obesity with bariatric surgery.
Type 1 Diabetes: A key area of study is type 1 diabetes, a form of diabetes that most often strikes in childhood and adolescence, thus placing particular burden on children and their families. Because the major forms of diabetes share many of the same devastating complications, type 1 diabetes research may potentially improve health outcomes of people not only with this disease, but also of those with type 2 diabetes.
Kidney Disease: The NIDDK is actively pursuing a range of research avenues on kidney disease, acute kidney injury, chronic kidney disease in children, hemodialysis, and other areas. Translating knowledge into practice, NIDDK is working with community health centers to improve screening and management practices, to enable better identification and treatment of people with chronic kidney disease before they develop kidney failure.
Health Care Impact: NIDDK research is of key importance to global health. Obesity and diabetes, for example, are of increasing importance in the developing world. Chronic hepatitis B is an important infectious disease in the U.S., but affects millions more worldwide. The Hepatitis B Research Network aims to improve the treatment and control of hepatitis B. These efforts are just a few examples of NIDDK’s broad spectrum of research areas that address the many chronic and debilitating diseases within its mission. The Institute also disseminates science-based health information through its Weight-control Information Network; the National Diabetes Education Program, which it co-sponsors with the Centers for Disease Control and Prevention; the National Kidney Disease Education Program; information clearinghouses; and other venues. The Institute also seeks to reinvigorate the biomedical research community through innovative programs such as the Medical Student Research Program in Diabetes, which is helping to attract a cadre of young physician scientists to study diabetes and obesity.
NIDDK will continue to seek external strategic planning and resource allocation advice from investigators, professional organizations, patient advocates, the public, NIDDK’s National Advisory Council, Interagency Coordinating Committees, ad hoc planning groups, and scientific conferences and workshops. NIDDK also plans to continue collaboration with other components of NIH and other federal agencies. Increasing knowledge and new technologies bring new opportunities for alleviating and conquering the diseases within NIDDK’s mission. NIDDK’s continuing goal is to build upon these emerging opportunities to improve public health, and its challenge for 2011 is to address them with new initiatives while preserving the investigator-initiated research portfolio.
Overall Budget Policy: The FY 2011 request for NIDDK is $2,007.589 million, an increase of $50.225 million or 2.6 percent over the FY 2010 enacted level. NIDDK is providing a 2 percent inflationary increase for non-competing and competing grants. In addition, NIDDK has targeted a portion of the funds available for competing research project grants to support high priority projects outside of the payline, including awards to new investigators, and early stage investigators. The Institute also seeks to maintain a balance between solicitations issued to the extramural community in areas that need stimulation and funding made available to support investigator-initiated projects. In FY 2011, NIDDK will support new investigators on R01 equivalent awards at success rates equivalent to those of established investigators submitting new R01 equivalent applications. Intramural Research and Research Management and Support receive increases to help cover the cost of pay and other increases. In addition, the NIDDK will support research consistent with the NIH Director’s Themes. Funds are included in R&D contracts to support several trans-NIH initiatives, such as the Therapies for Rare and Neglected Diseases program (TRND), the Basic Behavioral and Social Sciences Opportunity Network (OppNet), and support for a new synchrotron at the Brookhaven National Laboratory, as well as increased support for other HHS agencies through the program evaluation set-aside.
FY 2011 JUSTIFICATION BY PROGRAM
Program Descriptions and Accomplishments
Diabetes, Endocrinology, and Metabolic Diseases: The goals of this program are to increase understanding of diabetes and other diseases and disorders of the endocrine system and metabolism, and to develop and test potential prevention and treatment strategies. This program supports basic, clinical, and translational research, as well as research training, in the areas of type 1 and type 2 diabetes, cystic fibrosis, and other endocrine and metabolic disorders; obesity, neuroendocrinology, and energy balance; and development, metabolism, and basic biology of endocrine and metabolic tissues. Knowledge gained from research is broadly communicated to patients, health professionals, and the public through the support for the National Diabetes Information Clearinghouse and the National Diabetes Education Program. In FY 2009, the NIDDK-supported Diabetes Prevention Program Outcomes Study built upon Diabetes Prevention Program (DPP) research to establish the long-term durability of the DPP lifestyle and metformin interventions. Completed in 2009, the HEALTHY study—a multi-center, middle school-based study of strategies for reducing risk factors for type 2 diabetes in children launched in fall 2006—will provide a wealth of data on prevalence of overweight and obesity and diabetes risk factors in middle school population. Of the more than 6,300 students at the 42 middle schools around the country where the study was conducted who participated in the baseline examinations, 54 percent were Hispanic, 18 percent were African American, and 78 percent were eligible for free or reduced-price lunches. Ninety-nine percent of the enrolled children who remained in the participating schools at the end of the program completed the final examination. The Targeting Inflammation with Salsalate in Type 2 Diabetes clinical study completed its pilot phase and the full study began. Salsalate is an anti-inflammatory drug that is chemically similar to aspirin, but has fewer side effects. If successful, the study could lead to an effective, inexpensive way to treat type 2 diabetes. A new type 2 diabetes genetics study was launched to identify genes or gene regions conferring disease risk in minority populations. A new initiative seeks to foster multi-disciplinary research in diabetes, endocrinology, and metabolic diseases research. Finally, using ARRA funds, NIDDK promoted expansion and acceleration of research on diabetes, endocrinology, and metabolic diseases by awarding grants totaling more than $70 million in FY 2009. These included a grant to gain valuable insights into the way type 2 diabetes develops by studying uncommon genetic variants that can lead to the disease, and addition of funds to the Beta Cell Biology Consortium, to enable multidisciplinary research teams to pursue critical projects focused on two main goals: to clarify the genes, molecular pathways, and immune cells responsible for the autoimmune destruction of insulin-producing cells and to develop human insulin-producing cells to replace those destroyed by the autoimmune attack.
Budget Policy: The FY 2011 budget estimate for this program is $642.113 million, an increase of $16.512 million or 2.6 percent over the FY 2010 enacted level. With FY 2011 resources, the NIDDK will continue major diabetes clinical trials and encourage and support development of major new investigator-initiated clinical studies. FY 2011 funds will also support research capitalizing on new opportunities to identify diabetes risk genes in minority populations, to advance progress toward developing new therapeutic approaches, and to support comparative effectiveness research. NIDDK will also continue to fund translational research in FY 2011 and support health information dissemination activities to bring scientific discoveries in diabetes and obesity to real world medical practice and other community settings. In FY 2011, NIDDK will continue an initiative encouraging collaborative, multidisciplinary research teams to work on complex biomedical problems in diabetes, endocrinology, and metabolic diseases. NIDDK will also continue funding for centers advancing research relevant to diabetes and to cystic fibrosis and other genetic metabolic diseases. NIDDK plans for FY 2011 include capitalizing on new findings relevant to brown fat and gestational diabetes and pursuing other efforts as part of an overall balanced research portfolio.
Portrait of a Program: Diabetes Prevention Program Outcomes Study (DPPOS) and DEPLOY
DPPOS DEPLOY
FY 2010 Level: $12.720 Million* $0.567 Million
FY 2011 Level: $12.720 Million* $0.408 Million
Change: $ 0.000 Million -$0.159 Million
Over 23 million Americans have diabetes, and an estimated 57 million more have “pre-diabetes,” which places them at high risk of developing diabetes.[5] The landmark Diabetes Prevention Program (DPP) clinical trial demonstrated that a lifestyle intervention aimed at reducing weight through diet and exercise was an effective means to prevent or delay type 2 diabetes in people at risk. While the DPP lifestyle intervention was cost-effective, efforts are underway to find lower cost ways to test for pre-diabetes and deliver the lifestyle intervention more broadly in communities and at lower cost. Therefore, the DPP continues to drive discovery through follow-up studies and new trials that benefit from and expand upon the experience and findings from the DPP. To maximize benefits from its investment in the DPP, and to investigate the long term health outcomes of the interventions, the NIH is currently following the cohort of DPP patients through the DPP Outcomes Study (DPPOS). This study tracks DPP participants for an additional 10 years to assess the durability of the effect of the lifestyle intervention on weight loss, cardiovascular disease risk factors, and development of diabetes. A recently published paper from the DPPOS showed that 10 years after the intervention ended, the lifestyle intervention had reduced the rate of developing type 2 diabetes by 34 percent. Participants randomly assigned to make lifestyle changes also experienced improvements in measures of cardiovascular risk, including lower blood pressure and triglyceride levels, despite taking fewer drugs to control their heart disease risk. Examining longer-term benefits, beyond the average treatment period of 2.8 years in the DPP, has important implications for the cost-effectiveness of the intervention. Other critical ongoing research is aimed at translating findings from the DPP into more general practice, and further lowering the cost of intervention to encourage more health plans to cover this life-saving care. For example, the Diabetes Education and Prevention with a Lifestyle Intervention Offered at the YMCA (DEPLOY) study tests whether the intervention can be effectively and inexpensively delivered through YMCA programs. In this study, groups of 8 to 12 people who have pre-diabetes and other risk factors participate in a series of classroom-style meetings that focus on knowledge building and skill development to help them set goals, self-monitor, and problem-solve around their pre-diabetes. Major goals of the program include a five to seven percent reduction in baseline weight, and 150 minutes per week of moderate level physical activity similar to brisk walking. The NIDDK is also working with the Centers for Disease Control and Prevention (CDC) state diabetes programs to help translate the findings of DPP. These efforts are a key example of using science to contribute to health care reform, by establishing cost-effective approaches to preventing type 2 diabetes, a chronic disease with enormous human and financial costs. The estimated cost of diabetes in the U.S. in 2007 was $174 billion.[6]
*Includes $10.620 Million from NIDDK, $0.250 Million from NICHD, $0.800 Million from NIA, and $1.050 Million from NHLBI.
Digestive Diseases and Nutrition: The goals of this program are to increase understanding of digestive diseases, nutrition, and obesity, and to develop and test strategies for disease prevention and treatment. This program supports basic, clinical, and translational research, as well as research training, encompassing fundamental studies of the digestive system; disease-targeted research involving the esophagus, stomach, small intestine, large intestine and anorectum, liver and biliary system, and pancreas; studies relevant to nutrition; and research on obesity. Insights gleaned from scientific efforts are broadly communicated to patients, health professionals, and the public through the Institute’s National Digestive Diseases Information Clearinghouse and Weight-control Information Network. In 2009, the NIDDK expanded the Hepatitis B Clinical Research Network to 13 Clinical Centers, which are finalizing protocols to test treatments for chronic hepatitis B infection. NIDDK expanded and merged the Biliary Atresia Research Consortium and the Cholestatic Liver Disease Consortium to form the Childhood Liver Disease Research and Education Network to conduct studies on severe forms of childhood liver injury, including a new focus on liver disease associated with cystic fibrosis. The Institute-supported Adult to Adult Living Donor Liver Transplantation Cohort Study (A2ALL) was re-established with new clinical centers to continue to study the risks and benefits associated with liver transplants from living donors. The NIDDK extended the Clinical Outcomes Research Initiative and National Endoscopic Database, enhancing the largest national database on gastrointestinal endoscopy. NIDDK extended support of the Nonalcoholic Steatohepatitis Clinical Research Network as investigators complete two clinical treatment trials—one in adults and one in children—and continue to collect biospecimens and data from adult and pediatric patients with fatty liver disease not caused by alcohol. In a major new initiative, NIDDK funded projects of the Gastrointestinal Stem Cell Consortium to provide a better understanding of the biology and function of the intestine and aid in the development of therapies for intestinal diseases. These accomplishments and others are in line with the goals set forth in the research plan of the National Commission on Digestive Diseases finalized and disseminated in 2009. Studies from the NIDDK-sponsored Acute Liver Failure Study Group (ALFSG) were key to the development of new regulations regarding acetaminophen; other studies from the ALFSG demonstrated the benefits of N-acetylcysteine for treating some patients with acute liver failure that is not caused by acetaminophen poisoning. Finally, using ARRA funds, NIDDK promoted expansion and acceleration of research on digestive diseases, obesity, and nutrition by awarding grants totaling more than $63 million in FY 2009.
Budget Policy: The FY 2011 budget estimate for this program is $497.633 million, an increase of $12.792 million or 2.6 percent over the FY 2010 enacted level. In FY 2011, NIDDK will continue major clinical research networks to help understand and treat liver diseases, including hepatitis B, drug-induced liver injury, and nonalcoholic steatohepatitis. NIDDK will support a network to study immunosuppression in pediatric liver transplant recipients. Among its obesity-related efforts in FY 2011, NIDDK will support major ongoing observational studies to assess the health risks and benefits of weight-loss surgery in extremely obese adults and adolescents, as well as an ongoing trial evaluating the long-term health effects of weight loss in obese adults with type 2 diabetes (Look AHEAD). NIDDK will also use FY 2011 funds to support Digestive Diseases Research Core Centers, and to sustain a consortium that is conducting cutting-edge genetic research on inflammatory bowel disease (IBD). New research on intestinal stem cells that can benefit a variety of digestive diseases will continue in
FY 2011, along with other efforts as part of an overall balanced research portfolio.
Portrait of a Program: The Nonalcoholic Steatohepatitis Clinical Research Network (NASH-CRN)
FY 2010 Level: $4.000 Million*
FY 2011 Level: $4.000 Million*Change: $0.000 Million
Nonalcoholic steatohepatitis (NASH) accounts for 10 percent of newly diagnosed cases of chronic liver disease and ranks as one of the leading causes of cirrhosis in the United States. Characteristics of the disease include abnormal liver enzyme levels and fat accumulation in the liver along with liver cell injury, inflammation and fibrosis. While NASH typically occurs in middle-aged individuals who are obese and/or diabetic, in recent years it has been increasingly diagnosed in young people and even adolescents and children. Though most people with NASH feel healthy and show no outward signs of a liver disease, NASH can be progressive and lead to cirrhosis and end-stage liver disease, which may require liver transplantation. Currently, the only way to distinguish NASH from other forms of fatty liver disease is with a liver biopsy, and treatment options are limited. The NASH Clinical Research Network, consisting of eight clinical centers and a data coordinating center, was formed to address this problem by conducting research on the natural history, pathogenesis, and treatment of NASH. With the information collected from observational studies and clinical trials on both adult and pediatric NASH patients, the Clinical Research Network is building a database of information for use by researchers in the development of therapies for NASH. The Network also encourages collaborations among clinical and basic researchers to generate information and develop ancillary studies using the resources of the database, including genetic studies and studies of nutrition and eating habits. The Network is also conducting two prospective clinical trials of potential therapies. One of the trials is in adults, evaluating the safety and efficacy of the medication pioglitazone and the nutrition supplement, vitamin E, for their effects on the liver disease. A second clinical trial is in children and adolescents, comparing the medication metformin and vitamin E to placebo. Both of these trials are now completed and preliminary results demonstrate a clear effect of these approaches in lessening the liver injury in NASH. Renewal of funding for the Network has enabled expansion of the database to include samples from additional adult and pediatric participants and will allow for a second generation of clinical trials to further define the optimal therapy for this disease.
*Includes $3.500 Million from NIDDK and $0.500 Million from NICHD
Kidney, Urologic, and Hematologic Diseases: The goals of this program are to increase understanding of diseases and disorders of the kidneys, urinary tract, and blood (hematologic), and to develop and test potential prevention and treatment strategies. Basic, clinical, and translational research, as well as research training, is supported in the areas of chronic kidney disease, diabetic kidney disease, end-stage renal disease (kidney failure), polycystic kidney disease, and many other kidney diseases; urinary incontinence, benign prostatic hyperplasia, interstitial cystitis/painful bladder syndrome, stones, impotence, congenital urologic disorders, and urinary tract infections; and disorders of the blood and blood-forming organs including sickle cell disease, Cooley's anemia, hemochromatosis, and the anemia of inflammation and of chronic disease. Science-based information is communicated to patients, health professionals, and the public through NIDDK’s National Kidney and Urologic Diseases Information Clearinghouse and National Kidney Disease Education Program Which translates scientific knowledge into educational and clinical tools for patients from high risk populations and the health care providers who serve them. These tools are available at http://www.nkdep.nih.gov. In 2009, NIDDK initiated a chronic kidney disease biomarker consortium to find new predictive markers for progression of chronic kidney disease and associated cardiovascular disease. The NIDDK held a symposium on new directions in urinary incontinence research; scientific meetings on the genetics of vesicoureteral reflux and on urologic complications of diabetes and obesity; a strategic planning meeting to advance urological research; and a workshop on the development, physiology, and pathology of organ smooth muscle. NIDDK continued a multi-center consortium to study how acute kidney injury leads to or worsens chronic kidney injury and initiated a study to understand why arteriovenous fistulas -- surgically created connections between arteries and veins that facilitate hemodialysis -- do not always develop to be functionally suitable for dialysis. The National Kidney Disease Education Program expanded collaborative efforts with other federal agencies, particularly CMS and CDC, to reduce the burden of chronic kidney disease. Finally, using ARRA funds, NIDDK promoted expansion and acceleration of research on kidney, urologic, and hematologic diseases by awarding grants totaling more than $60 million in FY 2009. These grants included 31 2-year research project grants and 17 Challenge grants.
Budget Policy: The FY 2011 budget estimate for this program is $465.521 million, an increase of $11.961 million or 2.6 percent over the FY 2010 enacted level. In FY 2011, NIDDK will continue support for ongoing major clinical studies of chronic kidney disease in adults and children and fund new research to identify and validate biomarkers and risk assessment tools for patients with this condition. In FY 2011, NIDDK will continue treatment trials for polycystic kidney disease (HALT-PKD study) and continue support for the Consortium for Radiologic Imaging Studies of PKD. Centers focused on kidney, urologic, and hematologic research will receive continued funding, as will research on acute kidney injury and a study of arteriovenous fistulas. NIDDK will continue support for the Systolic Blood Pressure Intervention Trial (led by NHLBI) and for other efforts as part of an overall balanced research portfolio.
Portrait of a Program: Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease (CRISP) and Halt Progression of Polycystic Kidney Disease (HALT-PKD)
| | CRISP | HALT-PKD |
|---|
| FY 2010 Level: | $1.457 Million | $4.250 Million |
| FY 2011 Level: | | |
| Change: | $0.000 Million | $0.000 Million |
As many as one-half million people in the US and 4-6 million worldwide, are estimated to have polycystic kidney disease (PKD). The most common form is called autosomal dominant PKD (ADPKD). Half of patients develop kidney failure, on average around age 54; 23,000 were on dialysis or had a transplant for kidney failure in 2003, making it the Nation’s fourth leading cause of end-stage renal disease. Currently there is no cure and no specific treatment for PKD. ADPKD is characterized by progressive enlargement of cyst-filled kidneys. To combat PKD, the NIDDK has funded two complementary studies—CRISP and HALT-PKD—to develop better monitoring and imaging approaches, and improvements in care for individuals with ADPKD. The Consortium for Radiologic Imaging Studies of PKD (CRISP) was established to develop innovative imaging techniques and analyses to follow disease progression that would be useful to evaluate treatments. This valuable cohort of patients has been monitored through an extension of the original study: CRISP II. The image analysis methods developed in CRISP are currently being implemented in HALT-PKD and have also been adopted by industry-sponsored PKD treatment trials. The HALT PKD Consortium was established to design and implement clinical trials of treatments that might slow the progressive loss of renal function in PKD. HALT-PKD is currently testing whether optimum blood pressure management, in combination with drugs that target the renin-angiotensin system, will slow disease progression. The NIDDK has supported extensive and ongoing data collection related to volumetric analysis of kidney images, genotyping, and surrogate marker analysis in the CRISP studies and HALT-PKD. These data and samples will be available to the research community through the NIDDK Repository.
Special Statutory Funding Program for Type 1 Diabetes Research: Complementing the efforts of the Diabetes, Endocrinology and Metabolic Diseases program, this special program’s goal is to foster improved treatment, prevention, and cure of type 1 diabetes and its complications through basic, clinical, and translational research framed around six scientific goals: identifying genetic and environmental causes of type 1 diabetes ($54.400 million); preventing or reversing the disease ($35.734 million); developing cell replacement therapy ($30.266 million); preventing or reducing hypoglycemia ($7.231 million); preventing or reducing health complications ($6.803 million); and attracting new talent and applying new technologies to research ($15.566 million) (dollars are FY 2011 estimates). Although focused on type 1 diabetes, aspects of this research will also benefit those with other autoimmune disorders, as well as those with type 2 diabetes. Both type 1 and type 2 diabetes share a basis in impaired function of the insulin producing beta cells of the pancreas along with the same possible complications, such as heart disease, stroke, blindness, kidney failure, nerve damage, and lower limb amputations. The NIDDK-led Type 1 Diabetes TrialNet clinical trial network reported that rituximab, a therapeutic agent currently in use for non-Hodgkin’s lymphoma and rheumatoid arthritis, can substantially preserve the function of insulin-producing beta cells in people with recently diagnosed type 1 diabetes. The SEARCH for Diabetes in Youth study, a joint effort by the NIDDK and the Centers for Disease Control and Prevention, described the burden of diabetes in youth, providing population-based incidence and prevalence of diabetes in individuals younger than 20 years of age, stratified by race and ethnicity. Highlighting the need for improved therapeutics, SEARCH found high rates of poor blood sugar control and risk factors for cardiovascular disease, such as obesity, hypertension, and unhealthy blood lipid levels, although the rates of these co-morbidities varied by race and ethnic group. Scientists in the Institute’s Type 1 Diabetes Genetics Consortium have identified over 40 different genetic regions that influence a person’s risk of developing type 1 diabetes. A new initiative is investigating the function of these genes and gene regions and how they cause the disease. The Environmental Determinants of Diabetes in the Young study has completed screening nearly 400,000 infants for genetic risk factors for type 1 diabetes, enrolling over 7,350 to the study. Together with NICHD, the NIDDK initiated a new study of continuous glucose monitors (CGMs) to determine whether their use can help protect existing beta cell function in newly diagnosed type 1 diabetes, and released a new SBIR initiative to develop technologies to augment CGM technologies and develop an “artificial pancreas.”
Budget Policy: The FY 2011 budget estimate for the Special Statutory Funding Program for Type 1 Diabetes Research is $150.000 million, the same as FY 2010. NIDDK administers the program, but because of its trans-HHS nature, the resources are disbursed among multiple NIH Institutes and Centers as well as the CDC. Among ongoing NIDDK-led efforts that will continue with FY 2011 funds are an ambitious study that aims to identify environmental causes of type 1 diabetes in genetically susceptible individuals (TEDDY) ($37.400 million), and the Type 1 Diabetes TrialNet research network ($15.580 million). The Clinical Islet Transplantation consortium will also be supported in FY 2011 ($7.201 million). Research on development of an “artificial pancreas” will be continued in FY 2011 through initiatives funding small business research to develop new therapeutics and monitoring technologies for type 1 diabetes ($0.999 million) and clinical research on closed loop technologies. ($4.647 million).
Intramural Research: The goal of this program is to conduct basic, translational, and clinical biomedical research related to diabetes and other endocrine and metabolic diseases; digestive diseases, including liver diseases and nutritional disorders; obesity; kidney diseases; and hematologic diseases. Intramural research is conducted in the Institute’s laboratories and clinical facilities in Bethesda, Maryland, as well as in Phoenix, Arizona, where a long-standing research partnership with the Pima Indians in the region, who have the highest rates of type 2 diabetes in the world, has led to important scientific advances in type 2 diabetes and obesity. Research training is also an integral component of the Intramural Research Program (IRP). Recent results from the NIDDK IRP include the discovery that the gene MYH9 is a major contributor to the risk of non-diabetic kidney disease in African Americans, who are disproportionately burdened by kidney disease. Another recent IRP study identified seven distinct genomic regions affecting the probability of diabetic kidney disease. Because the study population was multiethnic, it was possible to show that some of these regions contribute to kidney disease in some groups, but not others. This year, installation of a trans-NIH 900 MHz nuclear magnetic resonance (NMR) facility, spearheaded by NIDDK, was completed. The instrument, funded in part by the Intramural Antiviral Target Program of the NIH Office of the Director, is shared by scientists from NIDDK, NCI, and NHLBI. This state-of-the-art instrument has played a key role in elucidating the structure of the fusion domain of the influenza virus (strain H3N1), with strain H1N1 currently being explored. Also, the instrument has yielded key information on the structure of HIV envelope protein gp41, a much-studied target that has resisted structure determination by other methods for over 20 years.
Budget Policy: The FY 2011 budget estimate for this program is $183.956 million, an increase of $5.704 million or 3.2 percent over the FY 2010 enacted level. With FY 2011 funds, the NIDDK Intramural Research Program will continue a broad spectrum of research studies to strengthen understanding of basic biology and disease mechanisms, and evaluate potential therapeutic approaches. For example, in FY 2011 intramural scientists will continue research on obesity in the trans-NIH Metabolic Clinical Research Unit, as well as research relevant to diabetes; digestive diseases, including liver disease; kidney disease; and hematologic disease. The program will also continue to support research training.
Research Management and Support: RMS activities provide administrative, budgetary, logistical, and scientific support in the review, award, and monitoring of research grants, training awards, and research and development contracts. RMS functions also encompass strategic planning, coordination, and evaluation of the Institute’s programs, regulatory compliance, international coordination, and liaison with other Federal agencies, Congress, and the public. Through its RMS activities, NIDDK has continued to fund meritorious basic, clinical, and translational research and research training efforts, and also continued its health information dissemination and education/outreach activities. Additionally, the NIDDK’s strategic planning, evaluation, and other activities have continued; some of these are highlighted above. In addition, ARRA resources allowed the Institute to support substantially more meritorious scientific research this year than in the past, and NIDDK rose to the management challenges related to funding this research.
Budget Policy: The FY 2011 budget estimate for RMS is $68.366 million (excludes Type 1 Diabetes), an increase of $3.256 million or 5.0 percent over the FY 2010 enacted level. NIDDK will continue effective research management and support so as to deploy research resources to the most meritorious and promising areas, and to communicate research opportunities and findings to investigators, health professionals, and the public.
Recovery Act Implementation
Recovery Act Funding: $445.393 million In FY 2009, the NIDDK received $445.393 million under the Recovery Act. Of this amount, $196.322 million was obligated in FY 2009 and $249.071 million will be obligated in FY 2010. These funds support two NIDDK Signature Initiatives, invest in new high-impact initiatives, and supplement ongoing projects. The “Novel Cell Therapies in Regenerative Medicine for Diabetes” Signature Initiative is investigating novel human islet cell replacement therapies for patients with type 1 diabetes. It is generally believed that replacement of insulin-producing pancreatic islet beta cells represents the ultimate treatment for type 1 diabetes. The “Genome-wide Association Studies and Replication in Diseases of Interest to NIDDK” Signature Initiative is identifying genetic variations associated with diseases within the NIDDK mission. High priority areas for this program include studies in minority populations and in diseases that have not been addressed in previous genome-wide studies. Once new genetic associations are identified, researchers can use the information to develop better strategies to detect, treat, and prevent disease. NIDDK Recovery Act funds also are supporting high-impact Challenge Grants in 11 topic areas, including stem cells, clinical research, translational research, and comparative effectiveness research. In addition, NIDDK funded Administrative Supplements to advance major research initiatives, including the Beta Cell Biology Consortium, the Halt Progression of Polycystic Kidney Disease (Halt-PKD) clinical trial, and the Action for Health in Diabetes (Look AHEAD) clinical trial. Administrative supplements to existing grants are funding additional personnel and investment in equipment and infrastructure that will accelerate the pace and achievement of scientific research. Supplements also were provided to current NIDDK grantees to foster research experiences for students and science educators over the summer months. In addition to creating jobs and accelerating grantee’s research, the latter program—which will be continued in 2010— increased science literacy, encouraged students to consider research careers and allowed science educators to participate in research conducted in NIH-funded laboratories. While stimulating the U.S. economy, the NIDDK ARRA funding should also stimulate a number of scientific areas that advance our public health mission. It is likely that exciting new findings resulting from this investment will open new areas of biomedical research.
Budget Authority by Object| | Total compensable workyears: | FY 2010
Estimate | FY 2011
PB | Increase or
Decrease |
|---|
| | Full-time employment | 630 | 658 | 28 |
| | Full-time equivalent of overtime and holiday hours | 2 | 2 | 0 |
| | Average ES salary | $163,547 | $165,837 | $2,290 |
| | Average GM/GS grade | 11.9 | 12.0 | 0.1 |
| | Average GM/GS salary | $94,133 | $95,451 | $1,318 |
| | Average salary, grade established by act of July 1, 1944 (42 U.S.C. 207) | $93,115 | $94,419 | $1,304 |
| | Average salary of ungraded positions | $123,858 | $125,592 | $1,734 |
| | OBJECT CLASSES:
Personnel Compensation: | FY 2010
Estimate | FY 2011
Estimate | Increase or
Decrease |
|---|
| 11.1 | Full-time permanent | $33,020,000 | $34,997,000 | $1,977,000 |
| 11.3 | Other than full-time permanent | 32,856,000 | 34,418,000 | 1,562,000 |
| 11.5 | Other personnel compensation | 1,635,000 | 1,652,000 | 17,000 |
| 11.7 | Military personnel | 2,019,000 | 2,048,000 | 29,000 |
| 11.8 | Special personnel services payments | 14,350,000 | 14,552,000 | 202,000 |
| | Total, Personnel Compensation | 83,880,000 | 87,667,000 | 3,787,000 |
| 12.0 | Personnel benefits | 18,831,000 | 19,823,000 | 992,000 |
| 12.2 | Military personnel benefits | 1,593,000 | 1,616,000 | 23,000 |
| 13.0 | Benefits for former personnel | 0 | 0 | 0 |
| | Subtotal, Pay Costs | 104,304,000 | 109,106,000 | 4,802,000 |
| 21.0 | Travel and transportation of persons | 2,200,000 | 2,232,000 | 32,000 |
| 22.0 | Transportation of things | 401,000 | 407,000 | 6,000 |
| 23.1 | Rental payments to GSA | 0 | 0 | 0 |
| 23.2 | Rental payments to others | 0 | 0 | 0 |
| 23.3 | Communications, utilities and | | | |
| | miscellaneous charges | 245,000 | 248,000 | 3,000 |
| 24.0 | Printing and reproduction | 575,000 | 587,000 | 12,000 |
| 25.1 | Consulting services | 1,153,000 | 1,169,000 | 16,000 |
| 25.2 | Other services | 15,515,000 | 15,695,000 | 180,000 |
| 25.3 | Purchase of goods and services from government accounts | 160,924,000 | 171,565,000 | 10,641,000 |
| 25.4 | Operation and maintenance of facilities | 2,825,000 | 2,848,000 | 23,000 |
| 25.5 | Research and development contracts | 102,797,000 | 101,809,000 | (988,000) |
| 25.6 | Medical care | 560,000 | 566,000 | 6,000 |
| 25.7 | Operation and maintenance of equipment | 3,980,000 | 4,029,000 | 49,000 |
| 25.8 | Subsistence and support of persons | 0 | 0 | 0 |
| 25.0 | Subtotal, Other Contractual Services | 287,754,000 | 297,681,000 | 9,927,000 |
| 26.0 | Supplies and materials | 14,500,000 | 14,649,000 | 149,000 |
| 31.0 | Equipment | 6,580,000 | 6,633,000 | 53,000 |
| 32.0 | Land and structures | 0 | 0 | 0 |
| 33.0 | Investments and loans | 0 | 0 | 0 |
| 41.0 | Grants, subsidies and contributions | 1,540,803,000 | 1,576,044,000 | 35,241,000 |
| 42.0 | Insurance claims and indemnities | 0 | 0 | 0 |
| 43.0 | Interest and dividends | 2,000 | 2,000 | 0 |
| 44.0 | Refunds | 0 | 0 | 0 |
| | Subtotal, Non-Pay Costs | 1,853,060,000 | 1,898,483,000 | 45,423,000 |
| | Total Budget Authority by Object | 1,957,364,000 | 2,007,589,000 | 50,225,000 |
Includes FTEs which are reimbursed from the NIH Roadmap for Medical Research
Includes Type 1 Diabetes Special Statutory Authority
Salaries and ExpensesOBJECT CLASSES:
Personnel Compensation: | FY 2010 Estimate | FY 2011 PB | Increase or
Decrease |
|---|
| Full-time permanent (11.1) | $33,020,000 | $34,997,000 | $1,977,000 |
| Other than full-time permanent (11.3) | 32,856,000 | 34,418,000 | 1,562,000 |
| Other personnel compensation (11.5) | 1,635,000 | 1,652,000 | 17,000 |
| Military personnel (11.7) | 2,019,000 | 2,048,000 | 29,000 |
| Special personnel services payments (11.8) | 14,350,000 | 14,552,000 | 202,000 |
| Total Personnel Compensation (11.9) | 83,880,000 | 87,667,000 | 3,787,000 |
| Civilian personnel benefits (12.1) | 18,831,000 | 19,823,000 | 992,000 |
| Military personnel benefits (12.2) | 1,593,000 | 1,616,000 | 23,000 |
| Benefits to former personnel (13.0) | 0 | 0 | 0 |
| Subtotal, Pay Costs | 104,304,000 | 109,106,000 | 4,802,000 |
| Travel (21.0) | 2,200,000 | 2,232,000 | 32,000 |
| Transportation of things (22.0) | 401,000 | 407,000 | 6,000 |
| Rental payments to others (23.2) | 0 | 0 | 0 |
| Communications, utilities and miscellaneous charges (23.3) | 245,000 | 248,000 | 3,000 |
| Printing and reproduction (24.0) | 575,000 | 587,000 | 12,000 |
| Other Contractual Services: | | | |
| Advisory and assistance services (25.1) | 1,153,000 | 1,169,000 | 16,000 |
| Other services (25.2) | 15,515,000 | 15,695,000 | 180,000 |
| Purchases from government accounts (25.3) | 101,041,000 | 105,792,000 | 4,751,000 |
| Operation and maintenance of facilities (25.4) | 2,825,000 | 2,848,000 | 23,000 |
| Operation and maintenance of equipment (25.7) | 3,980,000 | 4,029,000 | 49,000 |
| Subsistence and support of persons (25.8) | 0 | 0 | 0 |
| Subtotal Other Contractual Services | 124,514,000 | 129,533,000 | 5,019,000 |
| Supplies and materials (26.0) | 14,455,000 | 14,604,000 | 149,000 |
| Subtotal, Non-Pay Costs | 142,390,000 | 147,611,000 | 5,221,000 |
| Total, Administrative Costs | 246,694,000 | 256,717,000 | 10,023,000 |
Includes Type 1 Diabetes Special Statutory Authority
Appropriations History 1/| Fiscal Year | Budget Estimate
to Congress | House
Allowance | Senate
Allowance | Appropriation |
|---|
| 2002 | 1,457,915,000 | 1,446,705,000 | 1,501,476,000 | 1,563,833,000 |
| Rescission | | | | (453,000) |
| 2003 | 1,706,292,000 | 1,731,754,000 | 1,731,754,000 | 1,733,347,000 |
| Rescission | | | | (10,617,000) |
| 2004 | 1,820,000,000 3/ | 1,820,007,000 | 1,833,007,000 | 1,821,240,000 |
| Rescission | | | | (10,654,000) |
| 2005 | 1,877,696,000 3/ | 1,876,196,000 | 1,889,100,000 | 1,863,584,000 |
| Rescission | | | | (14,112,000) |
| 2006 | 1,872,146,000 3/ | 1,872,146,000 | 1,917,919,000 | 1,854,925,000 |
| Rescission | | | | (17,221,000) |
| 2007 | 1,844,298,000 3/ | 1,844,298,000 | 1,857,753,000 | 1,855,868,000 |
| Rescission | | | | 0 |
| 2008 | 1,858,045,000 3/ | 1,881,893,000 | 1,897,784,000 | 1,864,945,000 |
| Rescission | | | | (30,331,000) |
| Supplemental | | | | 9,077,000 |
| 2009 | 1,858,487,000 3/ | 1,767,071,000 | 1,755,881,000 | 1,911,338,000 |
| Rescission | | | | 0 |
| 2010 | 1,931,494,000 3/ | 1,974,251,000 | 1,940,518,000 | 1,958,100,000 |
| Rescission | | | | 0 |
| 2011 | 2,007,589,000 3/ | | | |
1/ Reflects enacted supplementals, rescissions, and reappropriations.
2/ Excludes funds for HIV/AIDS research activities consolidated in the NIH Office of AIDS Research.
3/ Includes Type 1 Diabetes Special Statutory Authority Funds.
Details of Full-Time Equivalent Employment (FTEs)| OFFICE/DIVISION | FY 2009 Actual | FY 2010 Estimate | FY 2011 PB |
|---|
| Office of the Director | 118 | 120 | 133 |
| Division of Diabetes, Endocrinology, and Metabolic Diseases | 27 | 27 | 27 |
| Division of Digestive Diseases and Nutrition | 22 | 22 | 23 |
| Division of Kidney, Urologic, and Hematologic Diseases | 19 | 19 | 19 |
| Division of Nutrition Research Coordination | 9 | 9 | 9 |
| Division of Extramural Activities | 52 | 52 | 53 |
| Division of Intramural Research | 379 | 381 | 394 |
| Total [*] | 626 | 630 | 658 |
| FTEs supported by funds from Cooperative Research and Development Agreements | (4) | (4) | (4) |
[*]Includes FTEs which are reimbursed from the NIH Roadmap for Medical Research
Average GM/GS Grade by Year| FISCAL YEAR | Average GM/GS Grade |
|---|
| 2007 | 11.6 |
| 2008 | 11.8 |
| 2009 | 11.8 |
| 2010 | 11.9 |
| 2011 | 12.0 |
Detail of Positions| GRADE | FY 2009 Actual | FY 2010 Estimate | FY 2011 PB |
|---|
| Total, ES Positions | 1 | 1 | 1 |
| Total, ES Salary | 159,683 | 163,547 | 165,837 |
| GM/GS-15 | 43 | 43 | 44 |
| GM/GS-14 | 60 | 61 | 62 |
| GM/GS-13 | 71 | 72 | 75 |
| GS-12 | 59 | 61 | 66 |
| GS-11 | 39 | 36 | 39 |
| GS-10 | 0 | 0 | 0 |
| GS-9 | 34 | 36 | 38 |
| GS-8 | 20 | 20 | 18 |
| GS-7 | 19 | 22 | 24 |
| GS-6 | 7 | 5 | 3 |
| GS-5 | 2 | 1 | 3 |
| GS-4 | 3 | 2 | 4 |
| GS-3 | 0 | 0 | 0 |
| GS-2 | 0 | 0 | 0 |
| GS-1 | 0 | 0 | 0 |
| Subtotal | 357 | 359 | 376 |
| Grades established by Act of July 1, 1944 (42 U.S.C. 207): | | | |
| Assistant Surgeon General | 1 | 1 | 1 |
| Director Grade | 10 | 10 | 10 |
| Senior Grade | 4 | 4 | 5 |
| Full Grade | 0 | 1 | 1 |
| Senior Assistant Grade | 3 | 2 | 1 |
| Assistant Grade | 0 | 0 | 0 |
| Subtotal | 18 | 18 | 18 |
| Ungraded | 271 | 273 | 285 |
| Total permanent positions | 365 | 367 | 384 |
| Total positions, end of year | 647 | 651 | 680 |
| Total full-time equivalent (FTE) | | | |
| employment, end of year | 626 | 630 | 658 |
| Average ES salary | 159,683 | 163,547 | 165,837 |
| Average GM/GS grade | 11.8 | 11.9 | 12.0 |
| Average GM/GS salary | 91,909 | 94,133 | 95,451 |
Includes FTEs which are reimbursed from the NIH Roadmap for Medical Research.
FY 2011 New Positions RequestedPosition | Grade | Number | Annual Salary |
|---|
Deputy Ethics Counselor | GS-0301-13 | 1 | 94,969 |
Management Analyst | GS-0344-13 | 1 | 89,033 |
Program Analyst | GS-0343-12 | 1 | 77,368 |
Grants Management Specialist | GS-1101-12 | 1 | 77,368 |
Lead Information Technology Specialist | GS-2210-14 | 1 | 105,211 |
Information Technology Specialists | GS-2210-13 | 6 | 89,033 |
Information Technology Specialists | GS-2210-12 | 2 | 74,872 |
Information Technology Specialist | GS-2210-11 | 1 | 62,467 |
Biologists | GS-401-12 | 8 | 74,872 |
Staff Clinician | AD-602-0 | 1 | 180,000 |
Senior Investigator - Branch Chief | AD-602-0 | 1 | 148,362 |
Tenure Track Investigators | AD-602-0 | 2 | 95,708 |
Clinical Fellow | AD-602-0 | 1 | 80,310 |
Tenure Track Investigator | AD-1310-0 | 1 | 92,001 |
Total Requested | | 28 | $1,341,574 |
Page last updated: February 01, 2010