

 E-mail Updates
E-mail Updates- Home
- Search for Research Summaries, Reviews, and Reports
EHC Component
- EPC Project
Full Report
- Research Review Jan. 31, 2012
Related Products for this Topic
- Research Protocol Oct. 19, 2010
- Disposition of Comments Report May 31, 2012
- Clinician Summary Apr. 16, 2012
- La Guías Sumaria de los Consumidores Jul. 31, 2012
- Executive Summary Jan. 31, 2012
Related Links for this Topic
Original Nomination


Consumer Summary – Apr. 16, 2012
Treating Chronic Pelvic Pain: A Review of the Research for Women
Formats
- View PDF (PDF) 648 kB
- Download Audio (MP3) 6.2 MB
- En Español
- Help with Viewers, Players, and Plug-ins
Table of Contents
- Is This Summary Right for Me?
- Understanding Your Condition
- Understanding Your Options
- Making a Decision About Treating CPP
- Source
Is This Summary Right for Me?
Yes, if:
A doctor* said you have chronic pelvic pain (pain in the area between your hips and below your belly button that has lasted 3 or more months).
No, if:
You sometimes have pain in your pelvis, but a doctor has not said it is chronic pelvic pain.
The pain you feel in your pelvis only happens during your period, sexual intercourse, urination, or bowel movements.
You are under 18 or male. This information is from research on adult women.
What will this summary cover?
This summary describes chronic pelvic pain and explains research about therapies for women with this condition. It can help you talk with your doctor about treating or managing chronic pelvic pain.
Researchers funded by the Agency for Healthcare Research and Quality (AHRQ), a Federal Government agency, reviewed 36 studies on therapies for chronic pelvic pain published between January 1990 and May 2011. You can read the report at www.effectivehealthcare.ahrq.gov/pelvicpain.cfm.
* In this summary, the term “doctor” refers to the health care professionals who may take care of you, including your physician, gynecologist, gastroenterologist, urologist, nurse practitioner, or physician assistant.
Understanding Your Condition
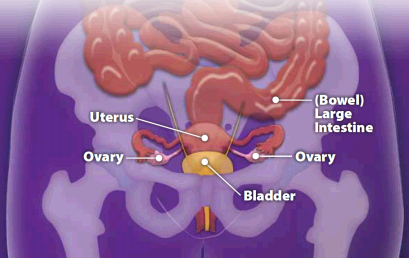
What is chronic pelvic pain?
Chronic pelvic pain (CPP) is ongoing pain in your pelvic area (the area between your hips and below your belly button) that lasts for 3 or more months.
- The pain may be dull, or it may be sharp and cramping.
- It may be constant, or it may come and go.
- The pain might not be in one specific spot and could be felt in your entire pelvic area.
- You may also feel pressure in your pelvic area.
- CPP can make it difficult to do daily activities or exercise.
What causes chronic pelvic pain?
CPP is a complex condition that can have many causes. It may be connected to other conditions. Some of these conditions include:
- Irritable bowel syndrome: A condition that affects your large intestine that can cause bloating, cramping, constipation, or diarrhea.
- Endometriosis (pronounced en-doh-mee-tree-OH-sis): The tissue from the lining of your uterus grows on the outside of that organ.
- Tense pelvic floor muscles: The muscles at the bottom of your pelvic area tense up or cramp.
- Painful bladder syndrome: Your bladder becomes sensitive and easily irritated.
- Scar tissue in the pelvic area: You may have scar tissue from an infection, an operation, or other treatment that now causes pain.
Finding the cause for your pelvic pain
There are treatments for specific causes of CPP. So it is very important to go to your doctor for a full workup to try to determine the cause of your CPP.
- Your primary doctor will ask you questions about your pain and your medical history and will give you a thorough physical exam.
- Your primary doctor may refer you to several different types of doctors: a gynecologist (a specialist in the female reproductive system), a gastroenterologist (pronounced gas-troh-en-tuh-ROL-uh-jist; a specialist in digestive tract diseases), or a urologist (a specialist in urinary tract diseases).
- These specialists will determine if the cause of your pain might be endometriosis, irritable bowel syndrome, or painful bladder syndrome. These are three common causes of CPP.
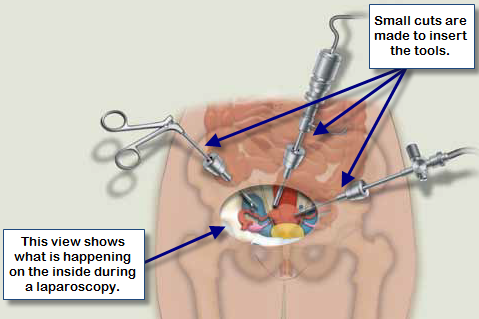
- Your doctor may suggest a diagnostic laparoscopy (pronounced lah-par-OS-koh-pee).
Laparoscopy may also be used in surgeries to treat your CPP or the condition that is causing your pain. More information about CPP surgeries with a laparoscope can be found below.
Understanding Your Options
Therapies for CPP
Very little is known about effective ways to treat CPP. Your doctor may try one or more ways to help relieve your pain or help you cope with it, but there is very little research to tell doctors which therapies work.
When a cause cannot be found, doctors may recommend a medicine, hormonal therapy, or surgery to try to relieve your CPP symptoms. Your doctor may suggest a narcotic or non-narcotic pain reliever such as aspirin, Tylenol®, Advil®, Demerol®, or OxyContin® to help manage your pain. In addition, your doctor may also suggest counseling, physical therapy, changes in your diet, or exercise to help with your CPP.
The table below tells what researchers have found out about how well medicines, hormonal therapies, and surgeries work to relieve CPP symptoms. Just because there is not enough research on many of the therapies listed does not mean that the therapies do not work for some people.
| Type of Therapy | What the Research Says |
|---|---|
| Medicines | |
|
|
| Hormonal Therapies | |
|
|
| Surgeries | |
|
|
What else should I know about treating CPP?
- There is no quick solution for CPP. You and your doctor may need to try many different therapies before your symptoms start to improve.
- Some therapy choices may take a long time before you start to feel better. It is important to not give up just because you do not see instant results.
- It is also important to try to stay positive while working with your doctor to manage your CPP. Let your doctor, friends, and family know when you feel discouraged.
Making a Decision About Treating CPP
What should I think about?
- When there is not much evidence to guide the decision you and your doctor need to make, your own wishes and values have an important role. You and your doctor should discuss:
- The possible side effects of medicines and which side effects you are willing to tolerate if a medicine may help your pain.
- If you should try non-surgery therapies before surgery, since there is not much evidence that surgery will help relieve your pain.
- How you feel about a hysterectomy, if your doctor suggests this. You should think about how important becoming pregnant or not beginning menopause (if your ovaries are removed) is to you.
- Other ways to keep CPP from affecting your work, relationships, and daily life.
- All therapies for CPP may be covered differently by your health insurance plan, and you may have out-of-pocket costs.
- It is important to find additional support from friends, family, counselors, and others while you and your doctor work to find the right treatment.
Ask your doctor
Talk with your doctor about how much pain you feel and which treatment best fits your specific needs, wishes, and values. Ask your doctor:
- How will we decide which therapies to try?
- What are the side effects or risks of each therapy?
- How long will it take until I start to feel better?
- How will I know if surgery is really needed?
- What resources are available for me to get support while we try to find the right treatment?
Source
The information in this summary comes from the report Noncyclic Chronic Pelvic Pain Therapies for Women: Comparative Effectiveness, January 2012.
The report was produced by the Vanderbilt Evidence-based Practice Center through funding by the Agency for Healthcare Research and Quality (AHRQ).
Additional information came from the MedlinePlus® Web site, a service of the National Library of Medicine and the National Institutes of Health. This site is available at www.nlm.nih.gov/medlineplus.
This summary was prepared by the John M. Eisenberg Center for Clinical Decisions and Communications Science at Baylor College of Medicine, Houston, TX. It was written by Geetha Achanta, Ph.D., Amelia Williamson Smith, M.S., Thomas Workman, Ph.D., Ronald Young, M.D., and Michael Fordis, M.D. Illustrations were created by Douglas Alexander. Women with chronic pelvic pain reviewed this summary.
Return to Top of Page