 NCI NewsCenter
NCI NewsCenter NCI Budget Data
NCI Budget Data Visuals Online
Visuals Online NCI Fact Sheets
NCI Fact Sheets Understanding Cancer Series
Understanding Cancer Series
Surgery: Prostate Cancer Surgery
Laparoscopic surgeries, in which a surgeon performs procedures through small incisions in the abdomen wall, have led to less invasive cancer surgeries with decreased pain and faster recovery times for patients. Because of the reduced size of the incisions, hospital stays are often shorter, with some patients even able to go home the same day.
During laparoscopic surgery, several slim, cylindrical ports, called trocars, are inserted into the patient’s abdomen through small incisions. Long thin instruments, including a lighted camera called a laparoscope, are passed through the trocars and into the abdomen. These instruments include scissors, graspers, and other instruments modeled after the typical instruments used in traditional open procedures.
However, because the surgeon does not have direct contact with the patient’s organs, and instead relies on a camera and monitor to view inside the body, there are certain limitations to laparoscopic surgery. For one, the surgeon is limited by the range of motion of the instruments. Unlike the human hand and wrist, the laparoscopic tools can only move in certain directions, limiting the types of actions that can be performed. In addition, because the surgeons are relying upon a two-dimensional screen displaying a mirror image of the instruments and the patient’s anatomy, there is a loss of depth perception, and an impact on hand-eye coordination. A new alternative to laparoscopic surgery, which is increasing in popularity, is robot-assisted surgery.
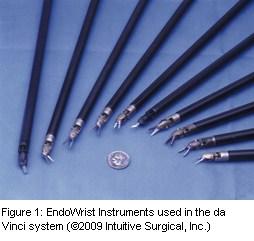
Surgery robots, which have been around in one form or another since the mid-1980s, can help surgeons overcome many of the challenges presented by the open or laparoscopic surgical styles, or platforms. Currently, the most successful and widely used surgical robot is the da Vinci system, developed by Intuitive Surgical in Sunnyvale, CA. The da Vinci system is similar to the laparoscopic surgical platform in that long, thin instruments resembling traditional surgical instruments (Figure 1) are inserted into the patient through trocars, allowing for smaller incisions, less pain, shorter hospital stays, and faster healing times. However, the style of the instruments and the way in which they are controlled are very different.
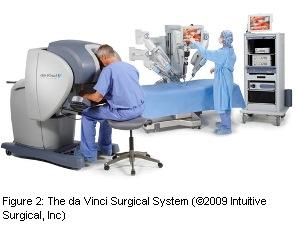
As shown in Figure 2, the da Vinci system has three main parts: the console, where the surgeon sits to operate the robot; the patient side cart, which is positioned over the operating table and contains the arms that hold the instruments; and a third cart which provides a view of the surgery for the other doctors and nurses in the room. When the surgeon looks into the console, he sees a three-dimensional view of the patients internal organs and the surgical instruments, similar to what he would see when operating in an open platform. Unlike when operating in the open platform, however, the viewer can magnify the image, using a high-resolution endoscopic camera. The console gives the surgeon more control over his own field of vision than is normally available using a laparoscopic platform, and there is no mirroring. In addition, because of its ergonomic design, the surgeon is not required to stand in awkward positions, for long hours, while using the long instruments required for laparoscopic surgery.

The arms of the robot on the patient cart and the individual instruments are operated by hand controls on the surgeon’s console (Figure 3) and foot pedals. Along with the magnification, the surgeon has the option of changing the scale of motion, so that the robot will reduce the amount of movement by a certain percentage. For example, if the surgeon moves his hand two inches, the robot can be set so that it will only move one inch. This is particularly useful for procedures needing extremely fine movements. The surgical robot also removes surgical tremor. In the open and laparoscopic platforms, if a surgeon’s hands shake slightly, that tremor will affect the instruments. However, with the surgical robot, those extremely small movements are not translated into the instruments.

Perhaps the largest advantage of the robot is in the design of the instruments. Unlike most laparoscopic instruments which can only move in certain directions, the da Vinci’s instruments are wristed. The surgeon can manipulate the instruments in multiple directions, giving the surgeon freedom similar to that of an open platform.
Students, as well as experienced surgeons who are new to the robotic platform, often learn on training machines that use models and inanimate objects to familiarize the trainee with the console and the use of the hand controls and foot pedals. Students can perform procedures, such as suturing and grasping, on foam circles and cones in order to become accustomed to the interface. This, of course, does not truly prepare the student for viewing anatomy through the console, so there are companies working to develop virtual reality models for the robot, to bridge the gap between operating on inanimate objects and operating on patients.
Robotic surgery and the da Vinci system are not without disadvantages. The largest disadvantage of robotic surgery is its cost. Currently, systems cost over $1 million and maintenance costs can be substantial. In addition, unlike operating in an open platform, the surgeon cannot feel the organs. When using the instruments to touch the organs, there is no tactile feedback, so surgeons must be extra vigilant about where each instrument is, in order to avoid damage to the organs. Finally, the da Vinci requires use of instruments that are manufactured only by Intuitive Surgical, Inc. If a procedure requires an instrument that is not currently available through the manufacturer, that part of the procedure must be completed by an assistant.
Surgical robots have been used in treating several cancers, including cancers of the lung, breast, gastrointestinal tract, kidneys, colon, rectum, bladder, prostate, testis, cervix, uterus, ovary, and tongue. The ability of this platform to blend benefits of both open and laparoscopic platforms has shown particular potential in the area of kidney cancer.
Application to Kidney Cancer
Peter A. Pinto, M.D., fellowship program director in the NCI’s Urologic Oncology branch, and colleagues, are pioneers in the use of robotic surgery for minimally invasive, nephron-sparing surgery, also called partial nephrectomy. While Dr. Pinto has been using the robot for radical prostatectomy (removal of the prostate) for quite some time, the use of the robot for partial nephrectomy is a new area of research.
The NCI Physician’s Data Query System lists several surgical treatment options for stage I renal cancer, including simple nephrectomy (removal of the kidney), radical nephrectomy (removal of kidney and surrounding tissues, glands and lymph nodes) and partial nephrectomy (removal of the tumor within the kidney and surrounding tissues, leaving the rest of the kidney intact). “Renal tumors that are less than or equal to 4 cm in size can be removed without removing the whole kidney – and you get the same cancer outcomes from a partial nephrectomy as you would if you took out the whole kidney,” explained Pinto. “But by leaving the healthy kidney behind, you decrease the risk of the patient going into renal insufficiency or renal failure… [which] can lead to heart problems… and shorten a person’s life.” However, in 2006, a study from the University of Michigan Medical Center reported that the use of partial nephrectomy to treat small, newly diagnosed kidney tumors was a vastly underutilized option across the country. In addition, at a meeting of the American Society of Clinical Oncology in 2008, researchers at the New York University School of Medicine reported that partial nephrectomy was offered as an option to only one out of every five patients who may have been eligible.
According to Pinto, one reason for this may be the difficulty of the procedure:
“In kidney surgery, the incision is… in the upper abdomen, often above the umbilicus [belly button]. It usually cuts through muscle, and occasionally cuts into the rib cage and you may have to remove part of the eleventh or twelfth rib, to get to the kidney. Those incisions are quite painful; and, unlike prostate surgery – which utilizes an open midline incision below the belly button and patients can go home in one or two days – open flank incisions, or kidney operations, often require a hospital stay of 3- 5 days or even a week. Laparoscopic kidney surgery has really improved, for the betterment of our patients, the recovery and pain and suffering from surgery, to the extent that laparoscopic renal surgery is now probably replacing open surgery for many of the smaller lesions.”
Pinto, along with his colleagues, W. Marston Linehan, M.D., Gennady Bratslavasky, M.D., and Craig Rodgers, M.D., in NCI’s Urologic Oncology Branch set out to apply the robotic platform to this issue – to overcome the difficulties involved in trying to complete a partial nephrectomy through a laparoscopic platform and to develop a way to educate other surgeons on this new found technique. In a 2007 paper, they demonstrated that, because of the wristed instruments, it was possible to complete all of the complex suturing and manipulation needed to achieve a minimally invasive partial nephrectomy using a robotic platform. “What we found was, in these patients who may have undergone a complete nephrectomy laparoscopically, or an open partial nephrectomy, we were able to successfully perform a robotic-assisted partial nephrectomy,” said Pinto. “They had their tumors removed, we were able to spare the kidney, we did it through minimally invasive small incisions, and they were able to go home very quickly.” They subsequently created an educational video for surgeons on this technique, and have been invited to several urological conferences to discuss these issues and train other surgeons.
While prostate surgery remains the most common cancer-related application of the robotic platform, many other fields within oncology have begun to explore its use, including gynecologic oncology. As robotic-assisted surgery rapidly develops and increases in popularity in the field of surgical oncology, Pinto stresses the importance of educating the next generation of surgeons in all three surgical platforms:
“I believe that most residency and fellowship programs do an excellent job in providing cases to our trainees that require they learn an open surgery skill set, a laparoscopic skill set, and a robotic skill set because when you are depending on technology, if it is not clear that it is going to work during the entire case you may have to move on to a different platform, whether it’s a laparoscopic platform or an open surgical platform…
“But I can see a time in the future when robotic assisted instruments become so common in the hospital, and there is more than one instrument available, that if the machine broke, you could just bring another one in during that procedure. But that day hasn’t come yet. Therefore, as a fellowship director here at NCI, I feel it necessary to train my fellows in all three aspects of surgery, which includes open, laparoscopic, and robotic.”
Works Cited
Miller, David C, John M Hollingsworth, Khaled S Hafez, Stephanie Daignault, and Brent K Hollenbeck. “Partial Nephrectomy for Small Renal Masses: an Emerging Quality of Care Concern?” The Journal of Urology, 2006: 853-858.
National Cancer Institute. “Partial Nephrectomy to Treat Small Renal Tumors Underused.” NCI Cancer Bulletin, February 19, 2008: 3-4.
National Cancer Institute. Renal Cell Cancer Treatment (PDQ®). May 22, 2008. http://www.cancer.gov/cancertopics/pdq/treatment/renalcell/ (accessed March 14, 2009).
Novakovic, Kristian R, and Peter A Pinto. “Robotic Surgery.” In DeVita, Hellman, and Rosenberg’s Cancer: Principles & Practice of Oncology, Eighth Edition, by Vincent T DeVita, Theodore S Lawrence and Steven A Rosenberg, 3021-3030. Philadelphia: Lippincott Williams & Wilkins, 2008.
Rogers, Craig G, Amar Singh, Adam M Blatt, W Marston Linehan, and Peter A Pinto. “Robotic Partial Nephrectomy for Complex Renal Tumors: Surgical Technique.” European Urology 53, no. 3 (Oct 2007): 514-21.
 Print This Post
Print This Post