Chapter 4Select Destinations
Safaris in East & Southern Africa
DESTINATION OVERVIEW
Arguably the ultimate in adventure travel, an African safari is also an easily doable family vacation, an experience of a lifetime for people of all ages, and with a little research, not much more difficult to arrange than a week at a Caribbean resort. While the centerpiece of safari-going remains viewing majestic animals in their natural habitats, many tour operators now include programs on local culture, history, geology, and ecosystems, and encourage travelers to get to know the people not merely as subjects of photos. Safaris can also be differentiated by the topography, vegetation, and bird life of the region. There are safaris for families, honeymooners, and people with similar interests (serious photography, for example). Animals can be viewed from open trucks, air-conditioned vans, private aircraft, hot air balloons, or while hiking—where animals are friendly. Accommodations range from crawl-in tents to portable, air-conditioned, walk-in tents with full bathrooms. And there are luxurious 5-star lodges with floodlit water holes to view animals at night. Lunch in the wilderness varies from prepackaged sandwiches eaten sitting on a tree stump to 3-course meals served on tables covered with linen cloths and matching napkins. Some safaris include side trips to exotic places, to see or climb Mount Kilimanjaro, visit Zanzibar, or view Victoria Falls, for example.
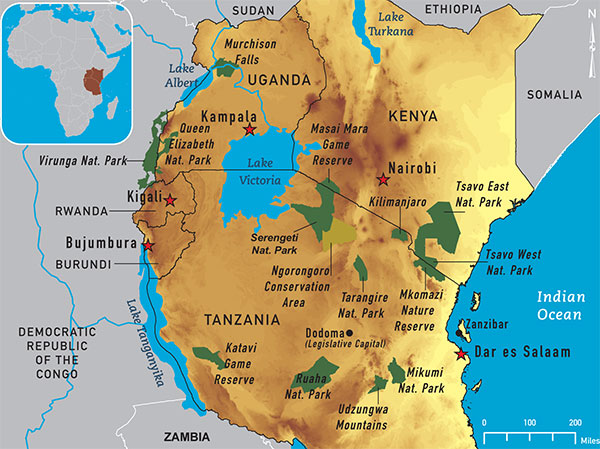
Travelers on their first safari often choose game parks in Kenya and Tanzania, in East Africa. The most famous game park in Kenya is the Masai Mara National Reserve, which, in effect, is the northern continuation of the Serengeti National Park game reserve in Tanzania, together forming the home of perhaps the grandest and most complete collection of the large wild animals for which Africa is famous. The Serengeti is the starting point of the annual migration of about 2 million wildebeest and several hundred thousand zebras as they search for pasture and water. Tanzania also has the Ngorongoro Crater, a 100-square mile depression (caldera) formed when a giant volcano, perhaps the size of Mount Kilimanjaro, exploded and collapsed on itself millions of years ago. The crater has most of the same animals as the Masai Mara reserve. In Southern Africa, popular safari destinations are in South Africa, Namibia, and Botswana. South Africa has Kruger National Park, one of the oldest, largest, and most visitor-friendly (much of it handicapped-accessible). Namibia’s best-known game reserve is the Etosha National Park, where the terrain consists of a bright white dry lake (salt pan). The Okavango Delta in Botswana is the world’s largest inland delta. Seasonally, rivers pour huge amounts of water into this area of the Kalahari Desert. The water has no outlet to the sea and evaporates in the intense heat. For more adventurous travelers, those willing and able to hike through dense rain forests and climb steep slopes, there is gorilla tracking in Rwanda and Uganda, with a good chance (but no promise) that gorillas will be sighted. There are only about 700 of them left in the world. Tours are limited to small groups and have many restrictions: no children and only 1 hour near the gorillas, for example. The major East and Southern African game parks are shown on Map 4-12 and some on Map 4-13.
Travelers should research the optimum time of the year for their safari. The wildebeest migration in the Serengeti is a seasonal event, for example, although the precise time of the migration may vary from year to year. Some parks have a dry season, offering better views of the animals, as the vegetation is sparser. And many areas of Africa have times of the year that are more comfortable for visitors, with cooler weather, less humidity, and less chance of rain.
HEALTH ISSUES
Health and safety issues that safari-goers are likely to encounter are mostly predictable and largely avoidable. The best insurance for carefree trips is a pre-travel consultation with a travel health provider. Advice must be itinerary- and game park-specific. Immunizations and preventive medications necessary for one park may not be necessary for others. Parks are thousands of miles apart and located in countries with different health standards, dissimilar climates, and at various altitudes. And health information for the country may not be sufficiently specific for a park within that country. Malaria, for example, may be a minor problem in South Africa and Namibia, but may be an issue at some parks in these countries, sometimes only seasonally. Generally, proper preparations, common sense precautions, the short duration of most trips (usually ≤2 weeks), experienced guides, leaving the driving to others, and spending little time in the large cities make safaris relatively low-risk undertakings for travelers of all ages.
Food and Water
Travelers’ diarrhea appears to be the most common ailment, and most cases are mild. Sensible food and water selections may reduce the incidence. Illness may occur even on deluxe trips. Carrying medication for self-treatment is generally recommended.
Animals
Wild animals are unpredictable. Travelers should follow oral and written instructions provided by safari operators. Animal-related injuries are extremely rare, usually the result of disregarding rules, for example approaching too closely to animals to feed or photograph them.
Rabies exists in most parts of Africa. While most cases result from bites and licks from dogs, all mammals can be rabid. All wounds from animals must be considered rabid until proven otherwise. Licks can result in rabies; the virus can enter through minor breaks in the skin, such as from insect bites, common in the tropics. In addition to rabies, bats can also transmit other diseases, such as viral hemorrhagic fevers, to humans. Travelers should be encouraged to avoid entering caves where bats are known to be present. Recent cases of Marburg fever have occurred in travelers who visited a “python cave” in western Uganda.
Malaria
Malaria transmission occurs in most major game parks. Most infections are caused by Plasmodium falciparum, and all P. falciparum in sub-Saharan Africa should be considered to be chloroquine-resistant. Safari activities often include sleeping in tents and observing animals at dusk or after dark, sometimes near water holes, all increasing the risk of being bitten by malaria-carrying mosquitoes. Taking appropriate preventive medication and using personal protection techniques—covering up with clothing, using insect repellents, and sleeping under permethrin-impregnated mosquito netting—are essential.
Yellow Fever
Yellow fever vaccination is recommended for virtually all parts of sub-Saharan Africa except those in Southern Africa (see Chapter 3, Yellow Fever and Malaria Information, by Country). Some countries require a valid yellow fever vaccination certificate as a condition of entry. Moreover, some safaris include more than one country. Travelers must check the requirements of each country on their itinerary. Some may require the certificate even if there is no yellow fever in the country travelers are leaving or entering.
Other Health Risks
Measures to prevent malaria help reduce the risk of 2 other, albeit rare, diseases among travelers: African tickborne fever and African trypanosomiasis. Tickborne fever occurs primarily in rural areas in Southern Africa. Symptoms include fever, localized lymphadenopathy, and rash. Prevention includes tucking pant legs into socks and daily “tick checks.” Trypanosomiasis (sleeping sickness) is transmitted by day-biting tsetse flies (Glossina). Wearing light-colored clothing seems to deter the flies. Insect repellents are only partially effective. Symptoms include fever, eschar at the site of the bite, headache, and signs of central nervous system involvement.
Myiasis and tungiasis are rare skin diseases. Myiasis is caused by fly larvae penetrating the skin and causing a boil-like lesion with a central aperture. Eggs are usually laid on clothing left to dry outdoors and the larvae enter the skin when the clothing is worn. Clothing should be dried indoors or ironed before wearing. Tungiasis is caused by direct penetration of skin by sand fleas, causing small, painful nodules, often on the foot adjacent to toenails. Prevention includes wearing closed-toed footwear and not walking barefoot.
Schistosomiasis (bilharzia) infection is widespread throughout Africa. The snails exist only in freshwater ponds, lakes, and rivers. All freshwater sources should be considered contaminated. Swimming in the ocean or well-chlorinated pools is safe.
Symptoms of many diseases acquired in Africa may surface weeks and occasionally months later, sometimes long after the traveler has returned home. Informing physicians of recent trips helps them make more prompt diagnoses.
Other Safety Risks
Although being a crime victim is an unusual occurrence for those on safari, robbery, muggings, and carjacking may occur in major urban centers, notably Johannesburg, Nairobi, and Mombasa. Street muggings during the day and night are common. The rates of fatal motor vehicle accidents in sub-Saharan Africa are among the highest in the world. Within game parks, serious motor vehicle accidents are rare. The poor roads discourage speeding. However, travel in rural areas between parks is high risk, especially after dark. If at all possible, nighttime driving in sub-Saharan Africa should be avoided.
BIBLIOGRAPHY
- Durrheim DN, Braack L, Grobler D, Bryden H, Speare R, Leggat PA. Safety of travel in South Africa: the Kruger National Park. J Travel Med. 2001 Jul–Aug;8(4):176–91.
- Gautret P, Schlagenhauf P, Gaudart J, Castelli F, Brouqui P, von Sonnenburg F, et al. Multicenter EuroTravNet/GeoSentinel study of travel-related infectious diseases in Europe. Emerg Infect Dis. 2009 Nov;15(11):1783–90.
- Leggat PA, Durrheim DN, Braack L. Traveling in wildlife reserves in South Africa. J Travel Med. 2001 Jan–Feb;8(1):41–5.
- Meltzer E, Artom G, Marva E, Assous MV, Rahav G, Schwartzt E. Schistosomiasis among travelers: new aspects of an old disease. Emerg Infect Dis. 2006 Nov;12(11):1696–700.
- Sinha A, Grace C, Alston WK, Westenfeld F, Maguire JH. African trypanosomiasis in two travelers from the United States. Clin Infect Dis. 1999 Oct;29(4):840–4.
- Thrower Y, Goodyer LI. Application of insect repellents by travelers to malaria endemic areas. J Travel Med. 2006 Jul–Aug;13(4):198–202.
- United Nations office at Nairobi. Security advice for United Nations visitors to Kenya. Nairobi: United Nations office at Nairobi; 2005 [cited 2008 Jun 30]. Available from: http://www.unon.org/unoncomplex/security_advice.php.
- World Health Organization. Global status report on road safety: time for action. Geneva: World Health Organization; 2009. Available from: http://www.who.int/violence_injury_prevention/road_safety_status/2009/en/.
Contact Us:
- Centers for Disease Control and Prevention
1600 Clifton Rd
Atlanta, GA 30333 - 800-CDC-INFO
(800-232-4636)
TTY: (888) 232-6348 - New Hours of Operation
8am-8pm ET/Monday-Friday
Closed Holidays - Contact CDC-INFO

{kind=link}