
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Agency for Health Care Policy and Research (US). AHCPR Consumer Guides. Rockville (MD): Agency for Health Care Policy and Research (US); 1992-1996.
This publication is provided for historical reference only and the information may be out of date.
What is Unstable Angina?
Unstable angina is a type of coronary artery disease. The coronary arteries bring oxygen-rich blood to your heart. Because your heart is a muscle, it needs oxygen to work well. In coronary artery disease, one or more of these arteries may be partially or even completely blocked.
The type of coronary artery disease you have usually depends on the amount of blockage in your arteries. A heart attack, called a myocardial infarction, means the heart muscle has been damaged by not getting enough blood. Stable angina usually does not damage the heart. Unstable angina is worse than stable angina and may progress to a heart attack if not treated.
Angina is caused by a lack of oxygen in the heart muscle. The symptoms of angina include pain or discomfort in the chest, arms, back, neck, or jaw. Sometimes, anginal pain may feel like a tightness or crushing sensation, or it may be a stabbing pain or seem like numbness. Some people mistake anginal pain as indigestion or gas pain.
Having either stable or unstable angina does not always mean you will have a heart attack. But, unstable angina can be serious and should be treated by a doctor.
Purpose of this Booklet
The purpose of this booklet is to describe unstable angina and how it relates to other heart conditions, answer some common questions about this condition, and describe the main types of treatments available.
This booklet is written for people who have been told they have unstable angina, have been treated before for coronary artery disease, or think they might have coronary artery disease. It is also for people with a family member or friend who has unstable angina or stable angina.
This booklet also suggests some questions to ask your doctor, as well as the best time to ask them.
How are Stable and Unstable Angina Different?
Anginal discomfort may be different for different people. Some people have anginal discomfort when they over-exert themselves (for example, when they shovel snow). Other people feel anginal pain when they get very upset or excited. Over time, they can usually tell which activities will give them discomfort. Usually, the discomfort will go away in a few minutes. This type of chest discomfort is called stable angina.
Stable angina attacks usually have a regular pattern. But in some people the pattern of angina is different-it becomes unstable.
People with unstable angina include those who:
Have anginal discomfort when they are resting or that awakens them from sleep.
Suddenly develop moderate or severe discomfort on exertion when they have never had angina before.
Have a marked increase in the frequency or severity of their discomfort.
Unstable angina is more serious than stable angina because the risk of having a heart attack is greater.
What Causes Unstable Angina?
In coronary artery disease, blockages -- made up of fats, such as cholesterol, and other debris -- form on the inside walls of the coronary arteries. In patients who have stable angina, the blockages may not seriously block the flow of blood.
In unstable angina, the blockages may be large. Sometimes, the blockage cracks open. When this happens, your body tries to heal the crack in the blockage by making a blood clot around the damage. If the clot is big enough to block the artery, the clot will keep blood flow from getting through. This can cause a heart attack.
Do I Need to See a Doctor?
This may depend on whether or not your doctor has ever told you that you have coronary artery disease.
If you have chest pain like that described on page 4 in the section "Chest Pain Can Be An Emergency," you should call an ambulance and then your doctor.
People Without Known Coronary Artery Disease
Many people do not know if they have heart disease. Any new or severe chest discomfort that is not related to an injury, such as a pulled muscle, could be unstable angina or a heart attack.
Unstable angina is not dangerous to most people who get medical care right away, but it can be very serious if it is not treated. Even anginal pain that goes away with rest can be serious. Only your doctor will be able to tell how serious it is and what should be done.
People with Known Coronary Artery Disease
If you have coronary artery disease, your past symptoms are the best guide to whether you should call your doctor about new symptoms. Call your doctor if the discomfort you are having is more severe or lasts longer than the discomfort you have had before, has begun to happen more frequently or with less effort, or happens when you are resting or asleep.
Chest Pain Can Be An Emergency
Here are some signs that your angina is very serious and you should go to the hospital right away:
Pain or discomfort that is very bad, gets worse, and lasts longer than 20 minutes.
Pain or discomfort along with weakness, feeling sick to your stomach, or fainting.
Pain or discomfort that does not go away when you take three nitroglycerin tablets (see page 11).
Pain or discomfort that is worse than you have ever had before.
If you live in an area where ambulance service is not quickly available, have someone drive you to the nearest hospital. You should not drive yourself to the hospital.
It is a good idea to talk with your family, friends, or neighbors about your heart condition and have them read this booklet. They should be familiar with warning signs that signal when you should go to the hospital. You also may want to tell them which medicines you are taking and where you keep them.
What Will Happen in the Emergency Room?
At your hospital emergency room, the doctors and nurses will decide if you have unstable angina. If you do have unstable angina, they will give you medicines through a vein in your arm to stop your pain and prevent injury to your heart. These medicines will help prevent blood clots and help your heart work more easily. You probably will be given oxygen to help you breathe and get more oxygen in your blood.
The doctors and nurses will ask how you are feeling and if the medicines have stopped your discomfort. It is important to tell them how you really feel. If the medicines do not stop your discomfort, there are other things they can do to help you.
These things need to be done quickly. The doctors and nurses may not be able to explain everything as it is happening. There will be time for you to ask questions after your doctor finds out how serious your condition is.
What is an Electrocardiogram?
When you are in the emergency room you may have an electrocardiogram, called an ECG or EKG. An ECG records on paper the electrical activity of your heart beat. The ECG may show your doctor if your heart muscle is getting enough oxygen-rich blood.
Will I Have to Stay in the Hospital?
Your ECG, past medical history, and the nature of your pain tell your doctor how serious your problem is.
If your doctor does not consider your condition to be serious enough to admit you to the hospital, he or she may make an appointment to see you in a day or two for more tests. If your chest discomfort comes back before this appointment and is like that described on page 4, "Chest Pain Can Be an Emergency," you should return immediately to the hospital.
It is not easy to accurately diagnose unstable angina, and your doctor may need to see you more than once to be sure.
If your doctor suggests admission to a hospital, you may be put in a regular bed or in an intensive care unit. In either case, treatment will continue while your doctor does more tests.
The tests you have will depend on how serious your condition is and how well the medicines control your discomfort.
What Tests Will I Have?
There is more than one kind of test your doctor can do to decide how badly your coronary arteries are blocked. Some of these tests are usually done while you are in the hospital. Other tests can be done in the hospital, but you do not have to stay overnight. Some tests can be done in your doctor's office.
Stress Tests
You may have an exercise tolerance test. In this test you will be asked to ride a stationary bicycle or walk on a treadmill while a doctor takes an ECG. Your doctor may give you an injection of a radioactive drug that shows up on special cameras. This allows your doctor to make pictures of how your heart moves and the way your blood flows.
This test will let the doctor see the changes that take place in your heart when you exercise. Trained personnel or the doctor will watch your condition by asking how you are feeling during the test. Be sure to follow their instructions carefully and tell them exactly how you feel.
If you have other health problems, you may be given another kind of stress test that does not use exercise. If you have this test, you will be given a special type of drug that makes your heart beat faster and opens your coronary arteries. An ECG will be taken at the same time. This test gives the doctor the same type of information as the exercise tolerance test.
The exercise tolerance test or other stress test will help your doctor tell how well your heart is functioning. Although stress tests are useful, they cannot tell your doctor exactly where your arteries are blocked or how bad the blockages may be. Also, these tests are accurate no more than 90 percent of the time. In some cases, doctors will want to do a cardiac catheterization.
Cardiac Catheterization
An angiogram or cardiac catheterization (sometimes called a cath) lets the doctor see the coronary arteries. A thin tube, called a catheter, is placed in an artery in either your arm or leg. The catheter is threaded up to your heart while your doctor watches on a screen.
The catheter will measure the blood pressure in your heart to see how well it is pumping blood. Then, a liquid is injected through the catheter into the artery, and x-rays are taken. The x-rays allow the doctor to see how much blockage there is and where it is located.
Cardiac catheterization is a test and not a treatment for unstable angina. A treatment called angioplasty looks and feels a lot like cardiac catheterization. Angioplasty is described on page 13.
What Can These Tests Show?
Stress testing may help your doctor decide how much of the heart could be in danger from blockages in your arteries. An angiogram shows how severe the blockages are and where they are. If you are told that you have single, two, or three-vessel disease, it means that one, two, or three of the major coronary arteries have a blockage. Your doctor may also talk about the percentage of blockage in the vessel.
The number of blocked arteries and the percentage of blockage are used to measure the severity of your coronary artery disease. Generally, the greater the number of vessels that are blocked, the higher the percentage of blockage, and the more poorly your heart pumps blood, the more severe the disease.
These tests will give your doctor a lot of information about your condition. At this point, he or she can start to give you more information about how serious your condition is and the types of treatment available.
Treatment of Unstable Angina
After your tests, you and your doctor can decide on which treatment you should have. The treatment that is best for you will depend on the results of your tests, whether or not you are still having discomfort, and your own preferences. In general you will have three choices: medical therapy, angioplasty, or bypass surgery.
Medical Therapy
You may have been given medicine in the hospital or emergency room. Some of these medicines, such as heparin which is used to decrease blood clotting, are given to you only in the hospital.
Many other medicines used to treat unstable angina can be taken at home. They come in the form of pills or creams that you can use by yourself.
Many people do very well on medicine alone. If you decide to use medicine to treat your unstable angina, and it does not control all your discomfort, you can still have bypass surgery or angioplasty later.
Almost everyone who has unstable angina will be given some type of medicine. The nurses or doctors caring for you will explain how and when to take all your medicines.
Several types of medicine can help to relieve the discomfort of unstable angina. Many of these drugs also make it easier for the heart to work. Medical therapy may be used alone or in combination with the other treatments described later in this booklet.
Medical therapy alone also may be the right treatment for people with other illnesses and people who do not want to have surgery or other procedures.
Medical therapy alone may benefit patients who:
Have a blockage or blockages in only one vessel
Have a less severe blockage
Do not have severe anginal discomfort
Have stabilized in the hospital
Here are some questions to ask your doctor about medical treatment.
What side effects will I have from the medicine?
Will I have to take medicine for the rest of my life?
Some people have uncomfortable side effects from the medicine, but most people feel better because they have less anginal discomfort. If you do have a reaction to a medicine, be sure to tell your doctor about it. Often the reaction goes away or becomes less severe with time. If not, your doctor may be able to change your medicine to make you more comfortable.
Remember, none of these drugs removes any of the blockages from your arteries. They do relieve anginal discomfort by bringing more blood to your heart or by making it easier for your heart to work.
Some of the most common medicines given to patients with unstable angina include aspirin, nitrates, and beta blockers.
Aspirin
How it works: Most people think of aspirin as something to relieve a headache or a fever. But aspirin also can prevent blood clots from forming. These are the same kind of blood clots that can block the coronary arteries and cause a heart attack.
Research in patients with unstable angina has proven that taking an aspirin every day reduces the risk of heart attack or death. Acetaminophen (for example, Tylenol [Trademark]) and ibuprofen (for example, Advil [Trademark]) are not the same as aspirin and should not be used in place of aspirin.
Side effects: Most patients with unstable angina will be told to take aspirin every day. Your doctor will tell you how much to take. When coated or buffered aspirin is used there are few major side effects. Aspirin should not be used if you are allergic to it or if you have had an ulcer or any other bleeding problem.
Nitrates
How they work: Nitrates (usually nitroglycerin and isosorbide) are used to open blood vessels. Nitrates increase blood flow to the heart muscle and the blood vessels and make it easier for the heart to work. Nitrates can relieve most anginal discomfort very quickly.
Nitrates come in tablets that you put under your tongue or a different type of tablet that you swallow, as a patch that you wear on your skin, or as a cream that you apply on your skin.
Nitrate tablets, cream, and patches all have a limited shelf life after which they will no longer work. Ask your pharmacist how long they will last and when you should replace them.
Nitrate cream and patches are for maintenance therapy only. If you are using a nitrate patch or cream, you should still use nitrate tablets if you have anginal discomfort.
Take one nitroglycerin tablet as soon as you feel discomfort. If the discomfort does not go away in 5 minutes, take a second tablet. If the discomfort does not go away after 5 more minutes, take a third tablet.
If the discomfort has not gone away after taking three tablets in 15 minutes, go to the hospital immediately. Do not wait!
Persistent discomfort that does not go away could be a sign that you are having a heart attack. You should see a doctor immediately.
Side effects: You may feel dizzy or lightheaded right after taking nitrates. Patients are usually told to take nitrate tablets while sitting down. Some people may also get a headache when they take nitrates.
Beta Blockers
How they work: This drug decreases the amount of work your heart has to do and the amount of oxygen your heart needs.
Side effects: Beta blockers are very powerful drugs that can have many side effects. About 10 percent of patients taking beta blockers will feel tired or dizzy. Depression, diarrhea, or skin rash may also happen in about 5 percent of patients. Mental confusion, headaches, heartburn, and shortness of breath are much less common.
Angioplasty
This procedure is done like an angiogram. A thin tube called a catheter is inserted into an artery in the groin and threaded up to the blocked artery. This catheter has a very small balloon attached on the end. When the catheter gets to the blockage, the doctor inflates the balloon. When the balloon is deflated, the blockage should be open enough for the blood to get through, stopping the anginal discomfort.
Benefits and risks of angioplasty
Possible benefits
Relieve anginal pain
Increase activity/exercise
Allow return to former activities
Reduce amount of medicine
Decrease anxiety/fear
Possible risks
Worsened angina
Emergency bypass surgery
Heart attack
Damage to the artery
Re-blockage of the artery
Death
Questions to ask your doctor about angioplasty include:
Will I need additional angioplasty or bypass surgery in the future?
What will it feel like to have angioplasty?
What is the chance that I might die during the angioplasty procedure or have other problems?
Bypass Surgery
Surgery is usually recommended for patients who have severe blockages in the left main coronary artery or disease in several vessels. Surgery is also an option when medicines do not control anginal symptoms.
Coronary artery bypass surgery can be a very effective way to increase the amount of blood getting to your heart and stop your discomfort.
In this operation, a piece of a vein, usually from your leg or an artery from your chest, is removed and used to "bypass" the section of your artery that has the most blockage. One end of the blood vessel is placed into your aorta. The aorta is the artery that supplies all the blood going out of your heart into your body. The other end is sewn into the artery below the blocked section to bypass the blockage.
Here are some questions to ask your doctor about bypass surgery:
What will it feel like to have bypass surgery?
Is it normal to be afraid of having surgery?
What is the chance that I might die during surgery or have other problems?
Will I need more surgery in the future?
Benefits and risks of coronary artery bypass surgery
Possible benefits
Prolong life
Relieve anginal pain
Increase activity/exercise
Allow return to former activities
Reduce need for medicine
Decrease anxiety/fear
Possible risks
Bleeding, requiring more surgery
Wound infection
Stroke
Blood clots
Organ failure (liver, kidney, lung)
Heart attack
Death
Angioplasty or Bypass Surgery?
Both angioplasty and bypass surgery are designed to do the same thing. They both can increase the supply of blood to your heart muscle. Depending on the severity of your disease, you may have a choice between the two.
How will you know which one is right for you? Your doctor will help you make this decision. But in general, angioplasty:
Is not as major a procedure as bypass surgery.
Results in a shorter hospital stay.
Will allow you to return to normal activities sooner.
You should also know that:
In about 2 to 5 percent of cases, angioplasty does not work, and emergency bypass surgery will be necessary.
About 40 percent of the time, the arteries become blocked again within 6 months of the angioplasty. If this happens, you may have to have angioplasty again or have bypass surgery.
Talking with Your Health Care Team
Some people think that their doctors are too busy to answer questions. Other people do not know how to ask their questions. But talking with the doctors, nurses, and other health care providers is an important part of your care.
Your questions are important, and the people taking care of you should make the time to answer your questions and listen to what you have to say. Your preferences for the type of treatment you receive are very important.
You may feel more comfortable if a family member or friend is there when you talk to your doctors, nurses, and other health care providers. This person can help to make sure that you understand what is happening, ask questions, and tell the doctor your concerns and preferences for care.
Here are some questions to ask your doctor before you decide what the best treatment might be for you.
Am I a candidate for medical treatment, angioplasty, or bypas surgery?
What are the chances that my arteries will become blocked again if I have angioplasty or bypass surgery? How soon might this happen?
Will I have to change my job or retire?
How soon can I resume my normal activities? What about resuming sexual activity?
How much will my treatment cost?
Do I have to go on a low-sodium or low-fat diet? If so, for how long?
Will I have a heart attack? Will I always have chest pain?
Can Blockages Come Back?
Neither angioplasty nor bypass surgery is a cure for coronary artery disease. Blockages continue to build up on artery walls even after angioplasty or bypass surgery.
Both angioplasty and bypass surgery can be repeated if the arteries become blocked again. The only way to stop coronary artery disease is to prevent the blockages from building up.
Although doctors do not know for sure why blockages form, they do know, from studies of large numbers of patients, that some people are more likely to have blocked arteries than others.
Your doctor may recommend that you attend a cardiac rehabilitation program. These programs usually are offered by local hospitals and very often they are covered by insurance. In a rehabilitation program, nurses, exercise specialists, and doctors will help you to change behaviors that put you at higher risk. They will also teach you how to exercise safely and help you gain confidence in your ability to live with heart disease.
Preventing blockages
The best way to prevent blockages from forming is to:
Take aspirin every day
Stop smoking
Eat foods that are lower in fat
Keep weight down
Increase physical activity
Control blood pressure if it is high
Lower stress
Living with Coronary Artery Disease
It is normal for you to worry about your health and your future. But, you should know that most people with unstable angina do not have heart attacks. Usually, angina becomes more stable within 8 weeks. In fact, people who are treated for their unstable angina can live productive lives for many years.
Coronary artery disease does not go away. Your behavior and lifestyle will affect your condition. This is why it is so important to follow the advice of your doctor and the other health care professionals who treat you.
Every year, thousands of people are told they have coronary artery disease. This may come as a shock, especially if they have never felt ill before. Often, they become anxious about their future and wonder if they will still be able to take care of their families or other responsibilities. It is normal to feel a loss of control, as if something has taken over your life.
Doctors, nurses, members of the clergy, and counselors all have experience in helping people with coronary artery disease. They can help you and your family. It is important to talk about how you feel, not just physically, but emotionally.
The best way to feel like you are in control is to learn more about coronary artery disease -- what it is and the choices you have. When you see your doctor or other health care provider, be prepared to ask questions.
How Can I Learn More About Unstable Angina?
Organizations that can provide additional information include:
American Heart Association
7272 Greenville Avenue
Dallas, TX 75231-4596
Phone: (800) AHA-USA1
National Heart, Lung, and Blood Institute Information Center
P.O. Box 30105
Bethesda, MD 20824
Phone: (301) 251-1222
The Mended Hearts, Inc.
7272 Greenville Avenue
Dallas, TX 75231-4596
Phone: (214) 373-6300
For Further Information
The information in this booklet was based on the Clinical Practice Guideline on Unstable Angina. The guideline was developed by a private-sector panel of experts, including physicians, surgeons, nurses, and people with unstable angina.
Support for this guideline was provided by the Agency for Health Care Policy and Research and the National Heart, Lung, and Blood Institute. Other guidelines on common health problems are available, and more are being developed.
For more information on guidelines or to receive another copy of this booklet, call toll free (800) 358-9295 or write to:
Agency for Health Care Policy and Research
Publications Clearinghouse
P.O. Box 8547
Silver Spring, MD 20907
Figures
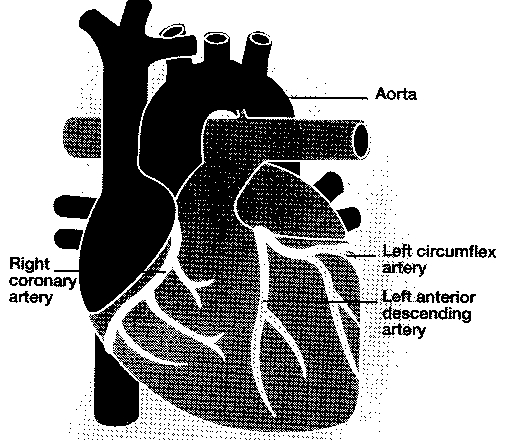
Outer view of heart showing the coronary arteries

Cross-section of a coronary artery showing blocked and normal sections
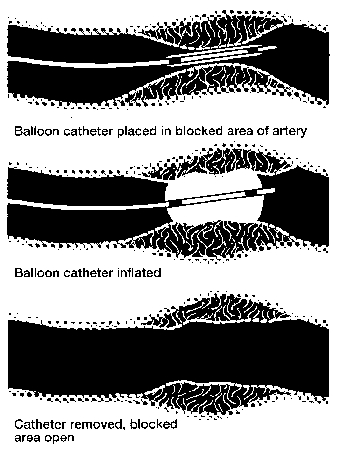
Cross-section of an artery showing how balloon angioplasty opens a blockage
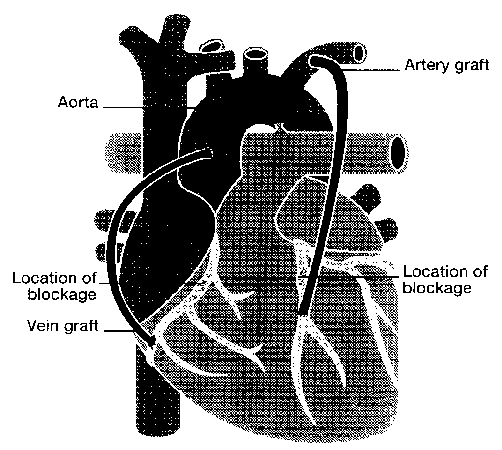
Outer view of heart showing how grafts are used to "bypass" blocked arteries
AHCPR Publication No. 94-0604.
National Library of Medicine DOCLINE Information: CAT/9423947
- What is Unstable Angina?
- Purpose of this Booklet
- How are Stable and Unstable Angina Different?
- What Causes Unstable Angina?
- Do I Need to See a Doctor?
- What Will Happen in the Emergency Room?
- What Tests Will I Have?
- What Can These Tests Show?
- Treatment of Unstable Angina
- Talking with Your Health Care Team
- Can Blockages Come Back?
- Living with Coronary Artery Disease
- How Can I Learn More About Unstable Angina?
- For Further Information
- Figures
-
Managing Unstable Angina: Patient and Family Guide - AHCPR Consumer Guides
Managing Unstable Angina: Patient and Family Guide - AHCPR Consumer GuidesBookshelf
-
Positron Emission Tomography (PET) for Oncologic Applications - Minnesota Health...
Positron Emission Tomography (PET) for Oncologic Applications - Minnesota Health Technology AssessmentsBookshelf
-
La insuficiencia cardíaca - AHCPR Consumer Guides
La insuficiencia cardíaca - AHCPR Consumer GuidesBookshelf
-
Lymphedema Pumps: Pneumatic Compression Devices - AHCPR Health Technology Review...
Lymphedema Pumps: Pneumatic Compression Devices - AHCPR Health Technology ReviewsBookshelf
-
Diagnostic Ultrasound Imaging in Pregnancy - NIH Consensus Statements
Diagnostic Ultrasound Imaging in Pregnancy - NIH Consensus StatementsBookshelf
Your browsing activity is empty.
Activity recording is turned off.
See more...