
|
| September 13, 2011 |
|
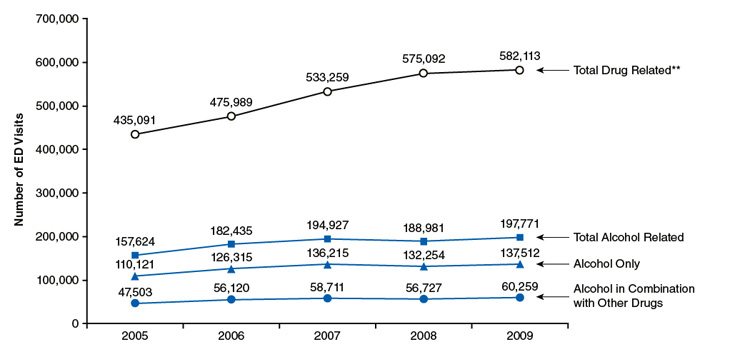
From 2005 to 2009, the number of drug-related ED visits among persons aged 12 to 20 significantly increased from 435,091 to 582,113 (Figure 1). Among patients aged 12 to 20, ED visits involving alcohol comprised one third of all drug-related ED visits in 2005 (36.2 percent, or 157,624 visits) and 2009 (34.0 percent, or 197,771 visits). The majority of alcohol-related ED visits among patients aged 12 to 20 from 2005 to 2009 involved alcohol only (110,121 visits in 2005; 137,512 visits in 2009). There was no significant change in the overall number of alcohol-related visits from 2005 to 2009, indicating no improvement in the trend for visits involving underage drinking.
|
| Type of ED Visit | 2005 | 2006 | 2007 | 2008 | 2009 |
|---|---|---|---|---|---|
| Total Drug Related** | 435,091 | 475,989 | 533,259 | 575,092 | 582,113 |
| Total Alcohol Related | 157,624 | 182,435 | 194,927 | 188,981 | 197,771 |
| Alcohol Only | 110,121 | 126,315 | 136,215 | 132,254 | 137,512 |
| Alcohol in Combination with Other Drugs | 47,503 | 56,120 | 58,711 | 56,727 | 60,259 |
| *ED visits for which age is unknown have been excluded from analysis. **The difference in the number of drug-related ED visits between 2005 and 2009 was statistically significant at the .05 level. Source: 2005 and 2009 estimates from the 2009 SAMHSA Drug Abuse Warning Network (DAWN). |
From 2005 to 2009, there was little progress in the reduction of alcohol-related visits among both adolescents and young adults. Furthermore, the number of alcohol-related ED visits changed little between 2005 and 2009 for most gender subgroups by age (Figures 2 and 3). Visits among male adolescents, male young adults, and female adolescents remained unchanged. There was an increase in alcohol-related visits of 38.3 percent from 2005 (37,218 visits) to 2009 (51,464 visits) by female young adults, reflecting the overall population growth of women aged 18 to 20.

|
| Type of ED Visits | 2005 | 2009 |
|---|---|---|
| Males Aged 12 to 17 | ||
| Total Drug-Related ED Visits** | 85,065 | 120,181 |
| Alcohol-Related ED Visits | 30,867 | 40,761 |
| Males Aged 18 to 20 | ||
| Total Drug-Related ED Visits** | 118,903 | 160,244 |
| Alcohol-Related ED Visits | 57,943 | 69,367 |
| *ED visits for which age is unknown have been excluded from analysis. **The difference in the number of drug-related ED visits between 2005 and 2009 was statistically significant at the .05 level. Source: 2005 and 2009 estimates from the 2009 SAMHSA Drug Abuse Warning Network (DAWN). |

|
| Type of ED Visits | 2005 | 2009 |
|---|---|---|
| Females Aged 12 to 17 | ||
| Total Drug-Related ED Visits | 122,617 | 139,603 |
| Alcohol-Related ED Visits | 31,587 | 36,155 |
| Females Aged 18 to 20 | ||
| Total Drug-Related ED Visits** | 108,405 | 161,901 |
| Alcohol-Related ED Visits | 37,218 | 51,464 |
| *ED visits for which age is unknown have been excluded from analysis. **The difference in the number of drug-related ED visits between 2005 and 2009 was statistically significant at the .05 level. Source: 2005 and 2009 estimates from the 2009 SAMHSA Drug Abuse Warning Network (DAWN). |
Between 2005 and 2009, the majority of alcohol-related ED visits among underage patients involved alcohol only for both adolescents and young adults. In 2009, adolescents made 54,726 visits that involved alcohol only, whereas young adults made 82,786 such visits (Figure 4). The trends for both adolescents and young adults showed modest—but not statistically different—increases between 2005 and 2009.
In 2009, there were an estimated 22,192 visits (8.5 percent of all alcohol-related visits) made by adolescents involving alcohol combined with another drug, while young adults made 38,067 such visits (11.8 percent of all alcohol-related visits). The trends for both adolescents and young adults did not show any statistical differences between 2005 and 2009.

|
| Age Group and Type of ED Visit | 2005 | 2006 | 2007 | 2008 | 2009 |
|---|---|---|---|---|---|
| Aged 18 to 20, Alcohol Only | 67,382 | 73,973 | 80,255 | 77,018 | 82,786 |
| Aged 12 to 17, Alcohol Only | 42,739 | 52,342 | 55,960 | 55,236 | 54,726 |
| Aged 18 to 20, Alcohol in Combination with Other Drugs | 27,784 | 31,702 | 32,308 | 36,975 | 38,067 |
| Aged 12 to 17, Alcohol in Combination with Other Drugs | 19,720 | 24,418 | 26,403 | 19,752 | 22,192 |
| *ED visits for which age is unknown have been excluded from analysis. Source: 2005 and 2009 estimates from the 2009 SAMHSA Drug Abuse Warning Network (DAWN). |
Each year, thousands of adolescents and young adults visit the ED for alcohol-related illnesses, injuries, and other problems. This report reveals little or no progress in reducing alcohol-related ED visits for this population, emphasizing the importance of concerted public health action to reduce underage drinking. Increased efforts to screen young people for alcohol and drug use and refer them for treatment may help reduce alcohol abuse and, in turn, the occurrence of such visits.
Communities can confront underage drinking problems by considering proven approaches such as policies and practices restricting youth access to alcohol, local media campaigns, and schoolbased curricula. It is critical to raise awareness about the dangers of underage drinking and to dispel cultural attitudes that support underage drinking as a "rite of passage."4 Although both young males and females can benefit from such initiatives, the growing population of young adult females, which has resulted in a greater number of alcohol-related ED visits for this group, warrants enhanced prevention and/or treatment efforts for this group.
The ED can be an effective venue for identifying the presence and severity of substance use disorders, and the ED visit experience can provide a stimulus for change. Guidelines for screening young people for alcohol problems have been developed, and alcohol screens for the ED have been evaluated.5,6 Research has shown that brief interventions in the ED help reduce abusive behaviors, which can also reduce the negative consequences of alcohol use.7 Such timely interventions in the ED can capitalize on "teachable moments" when the harmful consequences of substance use problems become apparent to patients and their families and challenge the common misconception that underage drinking is acceptable or an inevitable part of becoming an adult.
Referrals to appropriate substance abuse treatment programs that are geared to address treatment among young people are especially important, as is subsequent follow-up by primary care providers. Incorporating motivational interventions and matching other treatment components to individual needs can influence important behavioral changes. For example, approaches targeting adolescents that involve therapeutic communities or family therapy have been found to be successful in treating youths with substance use disorders.8
| The Drug Abuse Warning Network (DAWN) is a public health surveillance system that monitors drug-related morbidity and mortality. DAWN uses a probability sample of hospitals to produce estimates of drug-related emergency department (ED) visits for the United States and selected metropolitan areas annually. DAWN also produces annual profiles of drug-related deaths reviewed by medical examiners or coroners in selected metropolitan areas and States. Any ED visit related to recent drug use is included in DAWN. All types of drugs—licit and illicit—are covered. Alcohol involvement is documented for patients of all ages if it occurs with another drug. Alcohol is considered an illicit drug for minors and is documented even if no other drug is involved. The classification of drugs used in DAWN is derived from the Multum Lexicon, copyright 2010 Lexi-Comp, Inc., and/or Cerner Multum, Inc. The Multum Licensing Agreement governing use of the Lexicon can be found at http://dawninfo.samhsa.gov/drug_vocab. DAWN is one of three major surveys conducted by the Substance Abuse and Mental Health Services Administration's Center for Behavioral Health Statistics and Quality (SAMHSA/CBHSQ). For more information on other CBHSQ surveys, go to http://www.oas.samhsa.gov/. SAMHSA has contracts with Westat (Rockville, MD) and RTI International (Research Triangle Park, NC) to operate the DAWN system and produce publications. For publications and additional information about DAWN, go to http://DAWNinfo.samhsa.gov/. |
| The DAWN Report is published periodically by the Center for Behavioral Health Statistics and Quality (formerly the Office of Applied Studies), Substance Abuse and Mental Health Services Administration (SAMHSA). All material appearing in this report is in the public domain and may be reproduced or copied without permission from SAMHSA. Additional copies of this report or other reports from the Center for Behavioral Health Statistics and Quality are available online: http://oas.samhsa.gov. Citation of the source is appreciated. For questions about this report, please e-mail: shortreports@samhsa.hhs.gov.
DAWN_020 |
This page was last updated on December 11, 2010. |