| June 2, 2011 |
| June 2, 2011 |
|
Benzodiazepines are a class of central nervous system depressant drugs that are commonly prescribed for anxiety, insomnia, and seizure disorders.1 They were introduced in the late 1950s to replace barbiturates and other drugs that often had unwanted side effects, including a high addiction potential. It was not until almost 30 years later that the potential of benzodiazepines for abuse and dependence was recognized.
Benzodiazepines are often abused in combination with alcohol or other drugs (particularly opiates) to enhance or lengthen the high provided by the other substances or to offset their adverse effects.2,3 However, the abuse of benzodiazepines in combination with other substances can have severe and sometimes fatal consequences.4 Understanding the characteristics of admissions for benzodiazepine abuse can assist treatment providers in developing services that focus on the specific needs of these clients and help guide the development of effective prevention and early intervention programs that engage physicians, pharmacies, the pharmaceutical industry, and families. Additionally, this information can help raise awareness among physicians and provide them with a general profile of individuals who are at risk for abusing and becoming dependent on these substances.
This report uses data from the Treatment Episode Data Set (TEDS) for 2008 to examine the characteristics of substance abuse treatment admissions that reported any abuse of benzodiazepines, hereafter referred to as "benzodiazepine admissions." TEDS collects data on the primary substance of abuse at the time of admission to treatment and up to two additional substances of abuse at admission, subsequently referred to as "secondary substances of abuse." In 2008, benzodiazepines were reported as a drug of abuse by approximately 60,200 treatment admissions. While these admissions represented only 3.2 percent of all treatment admissions aged 12 or older, the proportion has grown since 1998, when benzodiazepines were reported by 1.3 percent (22,400) of all admissions aged 12 or older.
Demographic Characteristics
The majority of benzodiazepine admissions were male, between the ages of 18 and 34, and non-Hispanic White. Compared with all admissions, benzodiazepine admissions were more likely to be female (44.0 vs. 32.0 percent), more likely to be between the ages of 18 and 34 (55.3 vs. 44.5 percent), and more likely to be non-Hispanic White (84.8 vs. 59.7 percent) (Table 1). Only about one fifth (19.6 percent) of benzodiazepine admissions aged 16 or older were employed compared with 28.1 percent of all admissions aged 16 or older.
| Demographic Characteristic |
Benzodiazepine Admissions |
All Admissions |
||
|---|---|---|---|---|
| Total | 100.0% | 100.0% | ||
| Gender | ||||
| Male | 56.0% | 68.0% | ||
| Female | 44.0% | 32.0% | ||
| Age Group | ||||
| 12 to 17 | 5.1% | 7.5% | ||
| 18 to 24 | 22.7% | 18.5% | ||
| 25 to 34 | 32.6% | 26.0% | ||
| 35 to 44 | 21.2% | 24.2% | ||
| 45 to 54 | 14.8% | 18.7% | ||
| 55 or Older | 3.7% | 5.1% | ||
| Race/Ethnicity | ||||
| White, Non-Hispanic | 84.8% | 59.7% | ||
| Black, Non-Hispanic | 4.9% | 20.9% | ||
| Hispanic | 7.7% | 13.8% | ||
| Other | 2.6% | 5.6% | ||
| Employment Status (Aged 16 or Older) | ||||
| Employed | 19.6% | 28.1% | ||
| Unemployed | 43.3% | 36.7% | ||
| Not in Labor Force | 37.3% | 35.2% | ||
| Note: Percentages may not sum to 100 percent due to rounding. Source: SAMHSA Treatment Episode Data Set (TEDS), 2008. |
||||
Prior Use and Treatment History
Among benzodiazepine admissions that reported another substance of abuse at the time of admission, the majority (86.4 percent) indicated that they started using benzodiazepines after they first used the other substance, and the remaining 13.6 percent initiated use of benzodiazepines before initiation of the other substance of abuse. Nearly half of all benzodiazepine admissions (46.6 percent) reported daily use of benzodiazepines at treatment entry.
The most common source of referral to treatment was self-referrals (45.7 percent), followed by referrals from the criminal justice system (19.9 percent), alcohol or drug abuse care providers (17.0 percent), other health care providers (8.4 percent), and referrals from another source (9.0 percent). Compared with all admissions, benzodiazepine admissions were more likely to have had at least one prior treatment episode (70.5 vs. 56.6 percent); they were also more likely to have had three or more treatment episodes (36.8 vs. 23.0 percent).
The type of treatment services received differed between benzodiazepine admissions and all admissions. Benzodiazepine admissions were more likely to receive detoxification than all admissions (31.6 vs. 19.3 percent) and less likely to receive regular outpatient treatment (34.3 vs. 50.1 percent). Compared with all admissions, benzodiazepine admissions were more likely to have a psychiatric problem in addition to their substance use problem (43.4 vs. 24.9 percent).5
Abuse of Benzodiazepines in Conjunction with Other Substances
Compared with all admissions, benzodiazepine admissions were much more likely to report the abuse of another substance (95.0 vs. 54.4 percent). Of those benzodiazepine admissions that reported multiple substances of abuse, 82.1 percent reported primary abuse of another substance with secondary abuse of benzodiazepines, and 12.9 percent reported primary abuse of benzodiazepines with secondary abuse of another substance.
Older benzodiazepine admissions were generally more likely than those who were younger to report benzodiazepines as their only substance of abuse: 11.5 percent of benzodiazepine admissions aged 55 or older indicated that this was their only substance of abuse compared with about 3 to 5 percent of those aged 12 to 44 and 8 percent of those aged 45 to 54 (Figure 1). Conversely, younger benzodiazepine admissions were more likely than those who were older to report secondary abuse of benzodiazepines with primary abuse of another substance (around 80 to 85 percent of those aged 12 to 54 compared with about 74 percent of those aged 55 or older).
|
| Age at Admission | Primary Abuse of Benzodiazepines Only | Primary Abuse of Benzodiazepines with Secondary Abuse of Another Substance | Secondary Abuse of Benzodiazepines | ||||
|---|---|---|---|---|---|---|---|
| 12 to 17 | 3.5% | 11.4% | 85.1% | ||||
| 18 to 24 | 3.2% | 13.1% | 83.6% | ||||
| 25 to 34 | 4.3% | 12.4% | 83.3% | ||||
| 35 to 44 | 5.4% | 13.2% | 81.3% | ||||
| 45 to 54 | 7.6% | 13.3% | 79.1% | ||||
| 55 or Older | 11.5% | 14.8% | 73.7% | ||||
| Note: Percentages may not sum to 100 percent due to rounding. Source: SAMHSA Treatment Episode Data Set (TEDS), 2008 |
|||||||
Primary Benzodiazepine Admissions
Among the primary benzodiazepine admissions who reported multiple substances, the most commonly reported secondary substances were opiates, alcohol, marijuana, and/or cocaine. Overall, nearly one third of these primary benzodiazepine admissions reported secondary abuse of opiates (32.6 percent): specifically, 8.4 percent reported secondary abuse of heroin, and 25.3 percent reported secondary abuse of opiates other than heroin (primarily prescription pain relievers). About one quarter (27.6 percent) reported secondary abuse of alcohol, and 22.6 percent reported secondary abuse of marijuana. Fewer admissions reported secondary abuse of cocaine (15.6 percent) or other drugs (9.0 percent).
Secondary Benzodiazepine Admissions
Admissions who reported benzodiazepines as their second drug of choice most commonly reported the primary abuse of opiates, alcohol, marijuana, or cocaine. More than half of secondary benzodiazepine admissions reported primary abuse of opiates (54.2 percent): 29.8 percent of admissions reported primary abuse of heroin, and 24.4 percent reported primary abuse of opiates other than heroin. About one quarter (24.7 percent) reported primary abuse of alcohol, 11.4 percent reported primary abuse of marijuana, 6.3 percent reported primary abuse of cocaine, and 3.3 percent reported primary abuse of some other drug.
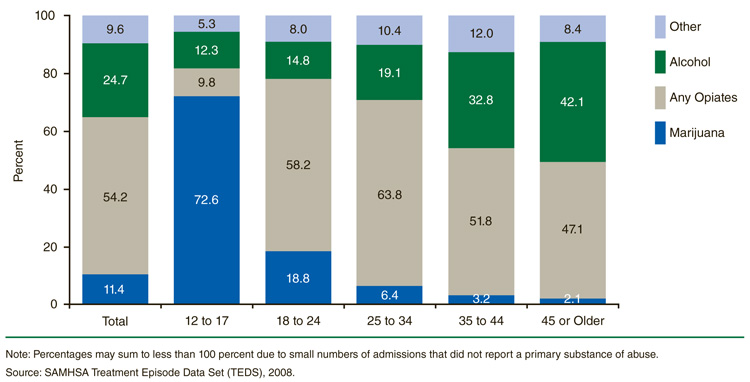
There was some variation in the primary drug of choice by age among the admissions who reported secondary abuse of benzodiazepines. While the majority of secondary benzodiazepine admissions aged 18 to 44 reported opiates as the primary substance, the older and younger age groups demonstrated different patterns. Opiates and alcohol were the most commonly reported primary substances of abuse among those aged 45 or older (47.1 and 42.1 percent, respectively) (Figure 2). Marijuana was the most commonly reported primary substance among those aged 12 to 17 (72.6 percent).
|
| Age at Admission | Other | Alcohol | Any Opiates | Marijuana |
|---|---|---|---|---|
| Total | 9.6% | 24.7% | 54.2% | 11.4% |
| 12 to 17 | 5.3% | 12.3% | 9.8% | 72.6% |
| 18 to 24 | 8.0% | 14.8% | 58.2% | 18.8% |
| 25 to 34 | 10.4% | 19.1% | 63.8% | 6.4% |
| 35 to 44 | 12.0% | 32.8% | 51.8% | 3.2% |
| 45 or Older | 8.4% | 42.1% | 47.1% | 2.1% |
| Note: Percentages may sum to less than 100 percent due to small numbers of admissions that did not report a primary substance of abuse. Source: SAMHSA Treatment Episode Data Set (TEDS), 2008. |
||||
Discussion
Abuse of prescription drugs, including benzodiazepines, is increasing across the country. Despite representing a small segment of the treatment population, the number of benzodiazepine admissions nearly tripled between 1998 and 2008, while overall admissions increased by only 11 percent. The data in this report, however, suggest multiple avenues for intervention and prevention of abuse of this powerful class of drugs. For example, since benzodiazepine abuse is most often a secondary substance of abuse, prescribing physicians may wish to screen for alcohol and other drugs of abuse and monitor patients more closely. Similarly, given the potential for abuse, patients using any of the 15 formulations of benzodiazepines should ensure that no one else has access to their medications and that they dispose of any leftover quantities in an appropriate manner. Programs that offer detoxification may also want to screen for secondary benzodiazepine abuse before beginning a program designed for opiate detoxification.
Additionally, a substantial proportion of benzodiazepine admissions have a psychiatric disorder in addition to their substance use disorder, and many may suffer from withdrawal symptoms (which can be severe) as they discontinue use. Screening and planning for mental health and medical issues early in the treatment process can help ensure that these issues can be effectively addressed. Finally, detoxification is often needed to address an individual's physical addiction to benzodiazepines; however, detoxification alone may not be sufficient for addressing all recovery needs. Following detoxification with a residential and/or outpatient treatment program may be vital for achieving full and lasting recovery.
End Notes
1 Benzodiazepines refer to drugs such as alprazolam (Xanax®), diazepam (Valium®), flurazepam (Dalmane®), triazolam (Halcion®), or similar drugs.
2 Knopf, A. (2011, January). Programs see sweeping increase in admissions for prescription opioids. Alcoholism and Drug Abuse Weekly, 23, 1-4.
3 Longo, L. P., & Johnson, B. (2000). Addiction: Part I. Benzodiazepines—Side effects, abuse risk and alternatives. American Family Physician, 61, 2121-2128.
4 National Institute on Drug Abuse. (2009, June). NIDA InfoFacts: Prescription and over-the-counter medications. Retrieved from http://www.drugabuse.gov/Infofacts/PainMed.html
5 Psychiatric problem in addition to alcohol or drug problem is a Supplemental Data Set item. The 31 States and jurisdictions in which it was reported for at least 75 percent of all admissions aged 12 or older in 2008—AL, AR, CA, CO, DE, FL, IA, ID, IL, KS, KY, LA, MD, ME, MI, MO, MS, MT, NC, ND, NE, NM, OH, OK, PR, RI, SC, SD, TN, UT, and WY—accounted for 52 percent of all such substance abuse treatment admissions in 2008.
Suggested Citation
Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. (June 2, 2011). The TEDS Report: Substance Abuse Treatment Admissions for Abuse of Benzodiazepines. Rockville, MD.
The Treatment Episode Data Set (TEDS) is a compilation of data on the demographic characteristics and substance abuse problems of those aged 12 or older admitted for substance abuse treatment. TEDS is one component of the Drug and Alcohol Services Information System (DASIS), an integrated data system maintained by the Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration (SAMHSA). TEDS information comes primarily from facilities that receive some public funding. Information on treatment admissions is routinely collected by State administrative systems and then submitted to SAMHSA in a standard format. TEDS records represent admissions rather than individuals, as a person may be admitted to treatment more than once. State admission data are reported to TEDS by the Single State Agencies (SSAs) for substance abuse treatment. There are significant differences among State data collection systems. Sources of State variation include completeness of reporting, facilities reporting TEDS data, clients included, and treatment resources available. See the annual TEDS reports for details. TEDS received approximately 1.9 million treatment admission records from 48 States, the District of Columbia, and Puerto Rico for 2008. Definitions for demographic, substance use, and other measures mentioned in this report are available in the following publication: Substance Abuse and Mental Health Services Administration, Office of Applied Studies. (December 11, 2008). The TEDS Report: TEDS Report Definitions. Rockville, MD. The TEDS Report is prepared by the Center for Behavioral Health Statistics and Quality, SAMHSA; Synectics for Management Decisions, Inc. (Arlington, VA); and RTI International (Research Triangle Park, NC). Information and data for this issue are based on data reported to TEDS through August 31, 2009. Access the latest TEDS reports at: |
The TEDS Report is published periodically by the Center for Behavioral Health Statistics and Quality (formerly the Office of Applied Studies), Substance Abuse and Mental Health Services Administration (SAMHSA). All material appearing in this report is in the public domain and may be reproduced or copied without permission from SAMHSA. Additional copies of this report or other reports from the Center for Behavioral Health Statistics and Quality are available online: http://oas.samhsa.gov. Citation of the source is appreciated. For questions about this report, please e-mail: shortreports@samhsa.hhs.gov. TEDS_028 |
This page was last updated on May 18, 2010. |