
|
| January 26, 2012 |
|
In 2009, pharmaceuticals were involved in 69,236 ED visits made by adolescents for medical emergencies associated with the misuse or abuse of drugs; of these, 14 percent (or 9,709 visits) involved narcotic pain relievers. The majority (72 percent) were made by patients aged 16 or 17, and 59 percent of visits were made by males (Figure 1).
 |
| Demographic Characteristic | Percent of ED Visits |
|---|---|
| Gender | |
| Male | 59% |
| Female | 41% |
| Age | |
| Aged 12 to 15 | 28% |
| Aged 16 to 17 | 72% |
| Source: 2009 SAMHSA Drug Abuse Warning Network (DAWN). |
Among ED visits by adolescents, the two most commonly identified types of narcotic pain relievers were oxycodone products (4,301 visits, or 44 percent) and hydrocodone products (3,771 visits, or 39 percent) (Table 1). The next most commonly involved narcotic pain reliever was methadone (887 visits, or 9 percent).
| Drug Category | Estimated Number of ED Visits | Percent of ED Visits* |
|---|---|---|
| Total ED Visits | 9,709 | 100% |
| Oxycodone Products | 4,301 | 44% |
| Hydrocodone Products | 3,771 | 39% |
| Methadone | 887 | 9% |
| Codeine Products | 641 | 7% |
| * Because multiple drugs may be involved in each visit, estimates of visits by drug may add to more than the total, and percentages may add to more than 100 percent. Source: 2009 SAMHSA Drug Abuse Warning Network (DAWN). |
An average of three substances were involved in narcotic pain reliever-related ED visits made by adolescents. About 23 percent of these visits involved one drug, 25 percent involved two drugs, 28 percent involved three drugs, 13 percent involved four drugs, and 10 percent involved five or more drugs. One in six visits (16 percent) involved two or more narcotic pain relievers.
Approximately half (53 percent) of ED visits also involved other pharmaceuticals (Figure 2). Among these, drugs used to treat anxiety and insomnia were the most common (38 percent, or 3,704 visits), followed by nonnarcotic pain relievers (9 percent, or 840 visits) (data not shown).
 |
| Drug Combinations | Percent of ED Visits |
|---|---|
| Combinations with Other Pharmaceuticals | 53% |
| Combinations with Illicit Drugs | 37% |
| Combinations with Alcohol | 17% |
| Combinations with Alcohol and Illicit Drugs | 8% |
| Combinations with Alcohol and Other Pharmaceuticals | 7% |
| * Because multiple drugs may be involved in each visit, percentages may add to more than 100 percent. Source: 2009 SAMHSA Drug Abuse Warning Network (DAWN). |
Illicit drugs were involved in 37 percent of ED visits. The most frequently identified illicit drug was marijuana (34 percent, or 3,325 visits).
Alcohol was involved in approximately 17 percent of visits. Alcohol and illicit drugs were combined with narcotic pain relievers in 8 percent of these visits while alcohol and other pharmaceuticals were combined with narcotic pain relievers in 7 percent of these visits.
Among narcotic pain reliever-related ED visits by adolescents, no significant differences between males and females were evident for visits involving pharmaceutical combinations (56 vs. 48 percent) or alcohol combinations (17 vs. 18 percent) (Figure 3). However, visits by males were more likely to combine illicit drugs with narcotic pain relievers than visits by females (46 vs. 25 percent), especially in visits involving marijuana (44 vs. 20 percent).
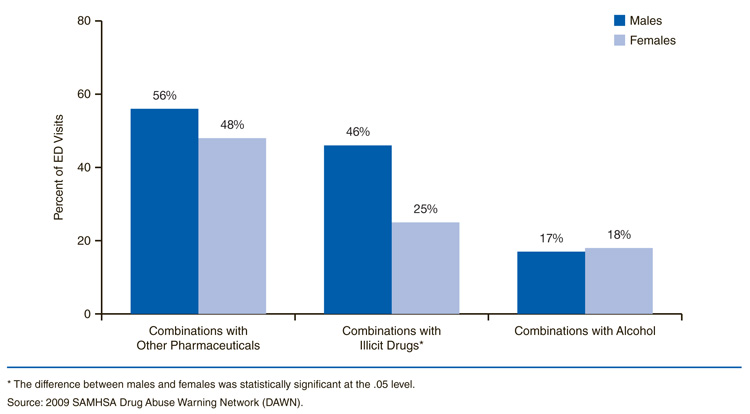 |
| Gender | Combinations with Other Pharmaceuticals | Combinations with Illicit Drugs* | Combinations with Alcohol |
|---|---|---|---|
| Males | 56% | 46% | 17% |
| Females | 48% | 25% | 18% |
| * The difference between males and females was statistically significant at the .05 level. Source: 2009 SAMHSA Drug Abuse Warning Network (DAWN). |
Because narcotic pain relievers are legally manufactured, regulated, and prescribed by physicians, adolescents may perceive their use as a less risky way to get high than using illicit drugs; however, misuse or abuse of these powerful medications can lead to dangerous health consequences.6 Raising awareness among health professionals regarding the magnitude of the problems associated with prescription drug misuse or abuse can help make prevention a priority in health care settings. Prior to prescribing narcotic pain relievers to adolescents, physicians should screen patients for substance abuse problems. All patients who are prescribed narcotic pain relievers should be instructed to safely store and dispose of the medication, especially if the patient's household includes adolescents or children.8 The ED visit may represent a particular opportunity for health care providers to educate patients and their family members about the dangers of the misuse or abuse of narcotic pain relievers and, if appropriate, provide referrals to treatment programs specializing in either adolescent substance abuse treatment and/or prescription narcotic drug addiction.
Substance use prevention programs targeting adolescents should work to dispel any myths regarding the safety of using these medications contrary to directions or without a prescription. Sharing any type of prescription medication, even with friends or relatives, should be discouraged. Community prevention efforts can begin with education campaigns that focus on the importance of preventing adolescents from accessing drugs that are not prescribed for them and encouraging parents and caregivers to store their pharmaceuticals in secure locations. Opening up a dialogue with adolescents about this problem may be especially important if an adolescent or a member of his or her family has been prescribed narcotic pain relievers. The Substance Abuse and Mental Health Services Administration (SAMHSA) has developed a toolkit to assist parents with these discussions, which can be accessed at the SAMHSA website: http://www.talkaboutrx.org/rxmonth2009_maximizing.jsp.
| The Drug Abuse Warning Network (DAWN) is a public health surveillance system that monitors drug-related morbidity and mortality. DAWN uses a probability sample of hospitals to produce estimates of drug-related emergency department (ED) visits for the United States and selected metropolitan areas annually. DAWN also produces annual profiles of drug-related deaths reviewed by medical examiners or coroners in selected metropolitan areas and States. Any ED visit related to recent drug use is included in DAWN. All types of drugs—licit and illicit—are covered. Alcohol involvement is documented for patients of all ages if it occurs with another drug. Alcohol is considered an illicit drug for minors and is documented even if no other drug is involved. The classification of drugs used in DAWN is derived from the Multum Lexicon, copyright 2010 Lexi-Comp, Inc. and/or Cerner Multum, Inc. The Multum Licensing Agreement governing use of the Lexicon can be found at http://www.samhsa.gov/data/DAWN.aspx. DAWN is one of three major surveys conducted by the Substance Abuse and Mental Health Services Administration's Center for Behavioral Health Statistics and Quality (SAMHSA/CBHSQ). For more information on other CBHSQ surveys, go to http://www.samhsa.gov/data/. SAMHSA has contracts with Westat (Rockville, MD) and RTI International (Research Triangle Park, NC) to operate the DAWN system and produce publications. For publications and additional information about DAWN, go to http://www.samhsa.gov/data/DAWN.aspx. |
| The DAWN Report is published periodically by the Center for Behavioral Health Statistics and Quality (formerly the Office of Applied Studies), Substance Abuse and Mental Health Services Administration (SAMHSA). All material appearing in this report is in the public domain and may be reproduced or copied without permission from SAMHSA. Additional copies of this report or other reports from the Center for Behavioral Health Statistics and Quality are available online: http://www.samhsa.gov/data/. Citation of the source is appreciated. For questions about this report, please e-mail: shortreports@samhsa.hhs.gov.
DAWN_038 |
This page was last updated on October 11, 2010. |