Emergency Department Visits Involving Nonmedical Use of Selected Pharmaceuticals
In Brief
According to the Drug Abuse Warning Network (DAWN) for 2004:
Nearly 1.3 million emergency department (ED) visits in 2004 were associated with drug misuse/abuse. Nonmedical use of pharmaceuticals was involved in nearly a half million of these ED visits.
Opiates/opioid analgesics (pain killers), such as oxycodone, hydrocodone, and methadone, and benzodiazepines, such as alprazolam and clonazepam, were each present in more than 100,000 ED visits associated with nonmedical use of pharmaceuticals in 2004.
Muscle relaxants, particularly carisoprodol and cyclobenzaprine, were involved in an estimated 26,000 ED visits related to nonmedical use.
Two thirds or more of ED visits associated with opiates/opioids, benzodiazepines, and muscle relaxants involved multiple drugs, and alcohol was one of the other drugs in about a quarter of such visits.
Public concern has been increasing about the nonmedical use of pharmaceuticals.1-3 The problem involves both medications available only by prescription and other pharmaceuticals, such as dietary supplements, that are commonly available over the counter. Medications with a high potential for abuse are being more widely employed in the treatment of chronic medical conditions.4-7 Some evidence also shows that increased long-term exposure may be associated with a higher likelihood of abuse.8 Recent epidemiological data have shown dramatic increases in nonmedical use of pharmaceuticals among youth (12 to 17) and older adults (i.e., 55+).9
The Drug Abuse Warning Network (DAWN), which collects data from a national sample of short-term, general, non-Federal hospitals,10 offers valuable information on the scope of this problem and the burden it creates on one segment of the health care system. Data on drug-related emergency department (ED) visits provide both an indication of the physical harm that may result from drug misuse and abuse as well as information about the characteristics of patients involved. An ED visit associated with drug misuse or abuse also represents a unique opportunity for health care providers to identify and refer patients for appropriate follow-up care, including substance abuse treatment. DAWN data on the disposition of these visits provide some evidence of how frequently such interventions occur as a result of care sought in EDs and the relative frequency of visits that do not receive such follow-up care.
This DAWN report examines drug-related ED visits associated with nonmedical use involving three types of pharmaceuticals that are often used nonmedically: opiates/opioid analgesics (pain relievers), benzodiazepines, and muscle relaxants. Nonmedical use includes taking a higher-than-prescribed or higher-than-recommended dose of a pharmaceutical, taking a pharmaceutical prescribed for another individual, malicious poisoning of the patient by another individual, and substance abuse involving pharmaceuticals.
Overview
According to DAWN data, there were over a half million ED visits involving nonmedical use of pharmaceuticals
in 2004 (Table 1). Of these visits, 32.2 percent involved opiates/opioids, 26.8 percent involved benzodiazepines,
and 4.8 percent involved muscle relaxants.
Table 1. ED visits involving nonmedical use of selected pharmaceuticals
Drug
Estimated visits
95% CI
Number
Percentage
Lower bound
Upper bound
Opiates/opioids
172,726
32.2%
136,497
208,956
Oxycodone/combinations
41,701
28,915
54,487
Hydrocodone/combinations
39,844
30,154
49,535
Methadone
38,806
28,151
45,461
Benzodiazepines
143,546
26.8%
110,329
176,764
Alprazolam
46,526
33,960
59,091
Clonazepam
28,178
21,721
34,635
Muscle relaxants
25,934
4.8%
19,647
32,221
Carisoprodol
14,736
10,047
19,426
Cyclobenzaprine
6,183
4,430
7,935
All ED visits involving nonmedical use of pharmaceuticals
536,247
100.0%
448,688
623,806
Note: CI = confidence interval.
Source: Office of Applied Studies, SAMHSA, Drug Abuse Warning Network, 2004 (03/2008 update).
An estimated 172,726 ED visits involved opiates/opioids. The most frequently listed opiates/opioids were oxycodone products (24.1% of opiates/opioids), hydrocodone products (23.1%), and methadone (21.3%). An estimated 143,546 ED visits involved benzodiazepines. Alprazolam and clonazepam, respectively, accounted for 32.4 and 19.6 percent of such visits. Carisoprodol was the most frequently named muscle relaxant (56.8% of the visits involving muscle relaxants).
Polydrug Use
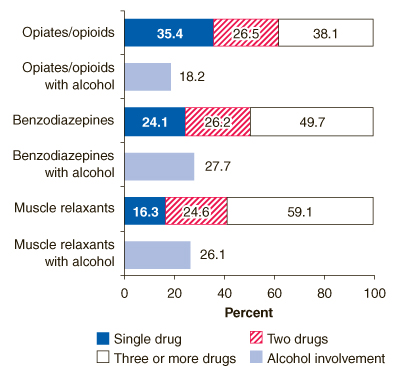
Typically, ED visits for nonmedical use of pharmaceuticals involve multiple drugs. Multiple drugs were involved in 64.6 percent of visits for opiates/opioids, 75.9 percent of visits for benzodiazepines, and 83.7 percent of ED visits for muscle relaxants (Figure 1). Often, alcohol is one of these other drugs. Alcohol was involved in 18.2 to 27.7 percent of visits involving opiates/opioids, benzodiazepines, or muscle relaxants.
Figure 1. Nonmedical use of pharmaceuticals alone and in combination
Figure 1 Table. Nonmedical use of pharmaceuticals alone and in combination
Single drug
Two drugs
Three or more drugs
Alcohol involvement
Opiates/opioids
35.4%
26.5%
38.1%
0.0%
Opiates/Opioids with alchohol
0.0%
0.0%
0.0%
18.2%
Benzodiazepines
24.1%
26.2%
49.7%
0.0%
Benzodiazepines with alcohol
0.0%
0.0%
0.0%
27.7%
Muscle relaxants
16.3%
24.6%
59.1%
0.0%
Muscle relaxants with alcohol
0.0%
0.0%
0.0%
26.1%
Source: a) U.S. Census Bureau; b) Office of Applied Studies, SAMHSA, Drug Abuse Warning Network, 2004 (03/2008 update).
Age
Patients aged 21 to 54 had the highest rates of ED visits for nonmedical use for all three drug classes (Figure 2). Within this age group, there was no statistically significant difference in the rates for individuals aged 21 to 34 and those aged 35 to 54, with the exception of patients aged 21 to 24 and patients aged 35 to 44 for muscle relaxants.
Figure 2. Rates of ED visits for selected pharmaceuticals, by age
Figure 2 Table. Rates of ED visits for selected pharmaceuticals per 100,000 population, by age
12-20
21-34
35-54
55+
Opiates/opioids
43
91
96
33
Benzodiazepines
46
76
80
21
Muscle relaxants
8
13
16
3
Source: Office of Applied Studies, SAMHSA, Drug Abuse Warning Network, 2004 (03/2008 update)
Discharge from the ED
Overall, about half of ED visits involving nonmedical use of opiates/opioids, benzodiazepines, or muscle relaxants ended with no evidence of follow-up care: ranging from 59.3 percent for opiates/opioids to 48.1 percent for benzodiazepines (Figure 3). Follow-up care is defined broadly to include referrals to detoxification or substance abuse treatment services, admission to an inpatient unit in the hospital, or transfer to another health care facility.
Figure 3. Discharge status of ED visits involving nonmedical use of selected pharmaceuticals
Figure 3 Table. Discharge status of ED visits involving nonmedical use of selected pharmaceuticals
No evidence of follow-up
Evidence of follow-up
Opiates/opioids
59.3%
40.4%
Benzodiazepines
48.1%
51.5%
Muscle relaxants
55.7%
44.3%
Source: Office of Applied Studies, SAMHSA, Drug Abuse Warning Network, 2004 (03/2008 update).
As a disposition from the ED, deaths accounted for less than 1 percent of visits. However, these estimates do not account for patient deaths occurring before reaching the ED, after admission to an inpatient unit, or after transfer to another facility.
Notes
McCabe, S. E., & Boyd, C. J. (2005). Sources of prescription drugs for illicit use. Addictive Behaviors, 30(7), 1342-1350.
Janofsky, M. (2004, March 18). Drug fighters turn to rising tide of prescription abuse. New York Times, Section A, p. 24.
Nonmedical use is defined as use of prescription-type drugs not prescribed for the respondent by a physician or used only for the experience or feeling they caused. Nonmedical use of any prescription-type pain reliever, sedative, stimulant, or tranquilizer does not include over-the-counter drugs.
Joranson, D. E., Ryan, K. M., Gilson, A. M., & Dahl, J. L. (2000). Trends in medical use of opioid analgesics. JAMA, 283(13), 1710-1714.
American Pain Society. (2003). Principles of analgesic use in the treatment of acute pain and cancer pain (5th ed). Glenview, IL: Author.
McQuay, H. (1999). Opioids in pain management. Lancet, 353(9171), 2229-2232.
Holbrook, A. M., Crowther, R., Lotter, A., Cheng, C., & King, D. (2000, January 25). Meta-analysis of benzodiazepine use in the treatment of insomnia. Canadian Medical Association Journal, 162(2), 225-233.
Chabal, C., Erjavec, M. K., Jacobson, L., Mariano, A., & Chaney, E. (1997, June). Prescription opiate abuse in chronic pain patients: Clinical criteria, incidence, and predictors. Clinical Journal of Pain, 13(2), 150-155.
National Institute on Drug Abuse. (2001; revised August 2005). Prescription drugs: Abuse and addiction. (NIH Publication No. 05-4881 & NIH Publication No. 01-4881, NIDA Research Report Series). Rockville, MD: U.S. Department of Health and Human Services, National Institutes of Health. [Available at
http://www.drugabuse.gov/ResearchReports/Prescription/Prescription.html]
Specialty hospitals, including children's hospitals, are not included in the DAWN sample.
The Drug Abuse Warning Network (DAWN) is a public health surveillance system that monitors drug-related morbidity and mortality. DAWN uses a probability sample of hospitals to produce estimates of drug-related emergency department (ED) visits for the United States and selected metropolitan areas annually. DAWN also produces annual profiles of drug-related deaths reviewed by medical examiners or coroners in selected metropolitan areas and States.
DAWN is one of three major surveys conducted by the Substance Abuse and Mental Health Services Administration's Office of Applied Studies (SAMHSA/OAS). For information on other OAS surveys, go to http://www.oas.samhsa.gov. SAMHSA has contracts with Westat (Rockville, MD) and RTI International (Research Triangle Park, NC) to operate the DAWN system and produce publications.
The DAWN Report is published periodically by the Office of Applied Studies (OAS), Substance Abuse and Mental Health Services Administration (SAMHSA). This issue was written by David Skellan (SAMHSA/OAS) with assistance from Scott Novak, Ph.D. (RTI International, a trade name of Research Triangle Institute), and Judy K. Ball, Ph.D., M.P.A. (SAMHSA/OAS). All material in this report is in the public domain and may be reproduced or copied without permission from SAMHSA. Citation of the source is appreciated.