0
0 slides
Return to Slide Library
Slides
Background: Coronary Heart Disease
Clinical Questions Addressed by the CER (1 of 2)
Comparative Adverse Effects of Oral Agents: CV Effects
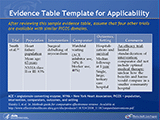
Evidence Table Template for Applicability
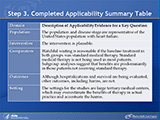
Step 3. Completed Applicability Summary Table
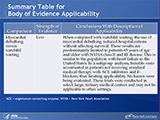
Summary Table for Body of Evidence Applicability
Comparative Effectiveness of Angiotensin-Converting Enzyme Inhibitors or Angiotensin II-Receptor Blockers Added to Standard Medical Therapy for Treating Patients With Stable Ischemic Heart Disease and Preserved Left Ventricular Systolic Function
Health Impact of Cardiovascular Disease in the United States (1)
Your slide tray is being processed.


 E-mail Updates
E-mail Updates